Organized by the Fields of Green for ALL with the support of the Veterans Action Council
Full recording available here
Myrtle Clarke, MD at Fields of Green for ALL: Fields of Green for ALL was established in 2013 to answer the need for extensive evidence to support our legal challenges on the road to the re-legalisation of cannabis in South Africa. We have been part of international drug policy civil society since attending UNGASS in 2016. We are proud of our victories along the way, but our work is far from done. We are joined by co-hosts the Veteran Action Council from the USA. The VAC is America’s only organisation campaigning for veterans access to alternative therapies, most notably but not exclusively, cannabis. We are grateful for the assistance of Michael Krawitz from the VAC for putting the side event together.
My civil society colleagues around the world and our cannabis family in South Africa have been an enormous source of strength since the murder of my partner Julian in July 2020. There has been no investigation into his murder, yet the South African police find the resources to continue to arrest and incarcerate citizens for cannabis offences every day in our country. In South African drug policy circles, we often use the statement that there will be no drug apartheid. It is a fact that cannabis can be the gateway to more rational policies around psychotropic plants and medicines. What is standing in the way of legal affordable access for millions across the world is evidence. The perceived harms of plants such as cannabis have never been fully substantiated by science. Traditional and legacy producers of plants such as cannabis are being left out of the newly created value chain of the medicinal cannabis industry. This is why we have come here to discuss today from the WHO Expert Committee on Drug Dependence to deliberations on a country level. The real evidence is being underplayed, misrepresented or just simply ignored. It is the very vulnerable people our conventions are designed to protect, who are bearing the brunt of this lack of evidence. Lack of evidence-based drug policies is the cause, and the effect is poverty, marginalisation and criminalisation resulting in human rights abuses across the globe. It is for this reason that we present three perspectives: a critique of the conventions and scheduling process, a look at cannabis in rural South Africa, the story of how kratom was nearly listed in the schedules, and a plea for evidence to be heard around the traditional coca plant.
Professor David Nutt travelled to South Africa in 2017 to be our principal expert witness in the trial of the plant. Our case against the South African government, which was unfortunately rendered part-heard when we ran out of court time. This was meant to be the showcase for the evidence around the use and cultivation of cannabis. In 2018, we achieved a Constitutional Court judgement declaring the prohibition of the personal use and cultivation of cannabis in private spaces unconstitutional. We are currently in talks with our governments around cannabis regulation, and we are proud to observe that our South African government is starting to take some of the evidence into account. But we still have a long way to go. The perfect expert to present the scientific evidence around the perceived harms of all drugs – coming to us today from the United Kingdom, Professor David Nuts.
Prof. David Nutt, Professor of Neuropsychopharmacology, Imperial College London: Good morning. My name is Professor David Nutt. I am a psychiatrist at Imperial College London and also the chair of the charity Drug Science in the UK. Today, I’m going to argue that there are some fundamental flaws in the current conventions. As you know, they have two goals: to prevent the abuse of psychoactive substances, and to ensure their availability for medical and scientific purposes. And I’m going to argue that they have failed to achieve both of those goals.
The decision-making criteria – the specified in the conventions relate to the substances liability to abuse and ill effects on health and its usefulness in medical therapy (in effect, whether there are adequate less abused alternatives). Of particular concern to me is that there appears never to have been any overt discussion over the possible negative impacts of scheduling, especially in relation to research, which I will show you was almost completely eliminated for a number of enormously important drugs and medicines on the next slide.
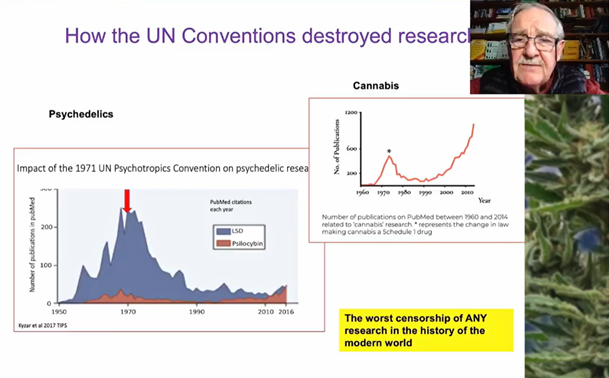
This graph on the left shows the impact of the UN 1971 Convention on Psychotropics in relation to research with LSD in blue and psilocybin in red. And you can see that following a peak around about 1970, research with these two psychedelic drugs virtually disappeared. And there were two reasons for that. The first is the failure of governments to fund research. The U.S. government is not funded, another study on LSD since that period. And secondly, when researchers were able to get funding from other sources, such as philanthropists, access to drugs for research was virtually banned by the regulators. A very similar profile was seen with cannabis. We’re following a big upsurge in research in the late 1970s. The imposition of international regulations had a very deleterious impact, which led to a period of about 20 years when research was effectively stifled. Pulling all this together, I’m going to argue that this is the worst censorship of any research theme in science or medicine in the history of the modern world. And it has been enormously deleterious to patients who are deserving of innovative medicines.
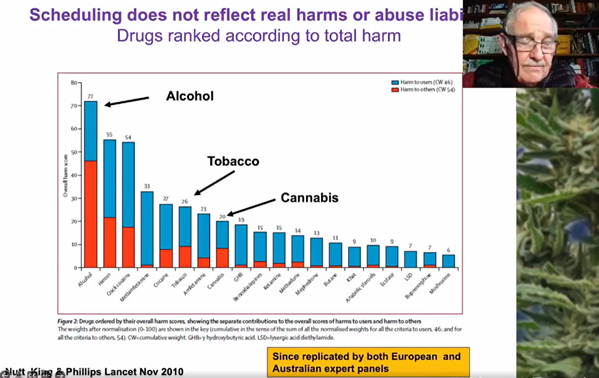
The second criticism of the scheduling is that it does not honestly and appropriately and fairly reflect real harms or real abuse liability. This is a graph of comparative harms in the UK of 20 different drugs published in The Lancet over ten years ago, showing that alcohol is the most harmful drug in the UK and that drugs like heroin, crack cocaine and methamphetamine are harmful but less so than alcohol. And that many of the drugs controlled under the Schedule I and Schedule IV of the UN Convention, such as LSD and magic mushrooms and MDMA have massively less harm, both to the individual – the blue bar, and to society – the red bar, than legal drugs like alcohol and tobacco, and other drugs such as opiates and amphetamines which are controlled under lower schedules, therefore allowing them to be medicines. This analysis was done by about 30 UK experts. It’s since been replicated by similar sized groups of both European and Australian experts. And it is universally accepted now that this represents a very robust and honest comparative assessment of the harms of different drugs, which clearly has no relationship with the current conventions. They are out of step with our best estimates of comparative harms.
Moreover, current scheduling does not reflect special benefits of some of the drugs which are banned. And which have now been shown difficultly because of their illegal status to have value in conditions. So for instance, cannabis has utility in pain spasticity and epilepsy, psilocybin in depression, addictions, cluster headaches, MDMA in PTSD and alcohol addiction.
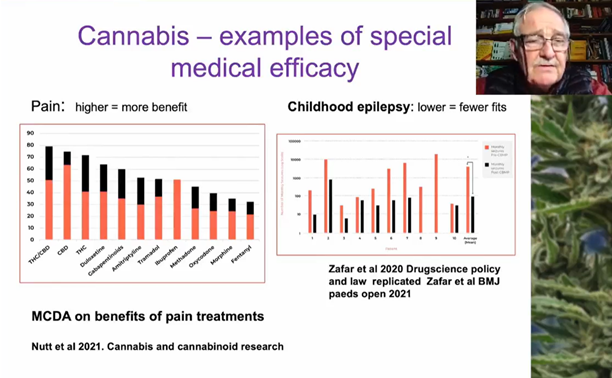
And the next few slides illustrate some examples of the unique special ability of these drugs. So starting first with medical cannabis. Here are two recent studies, both conducted by the Drug Science expert group. On the left, we have a multi-criteria decision analysis on the benefits of different treatments for chronic pain. And you see that combination of THC and cannabidiol scores highest in terms of benefits, followed by CBD, followed by THC. They exceed the benefits overall of alternative licensed medicines such as duloxetine, gabapentinoids and opiates such as methadone, morphine and fentanyl. On the right hand side, you see the impact of medical cannabis in children with severe treatment resistant, childhood epilepsy, many of whom have failed also on cannabidiol Epidiolex. And what you see here is the reduction in seizures from red to black in children given full plant extract cannabis and the difference in terms of monthly seizures was 50 times fewer seizures. This initial 2020 publication has since been replicated in 2021, with a further cohort of 20 children. There is incontrovertible evidence now that full spectrum medical cannabis can be transformational in the lives of children with severe treatment resistant epilepsy.
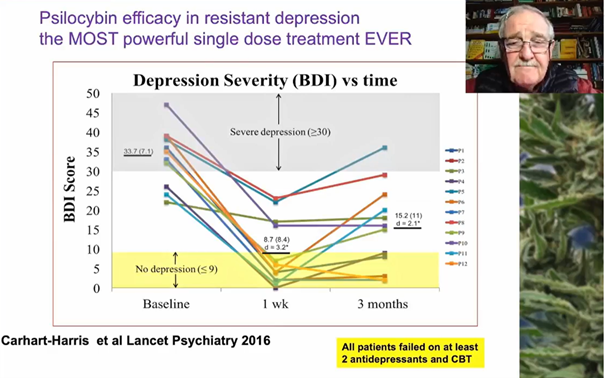
It was the first trial to show that psilocybin had profound efficacy in people with treatment resistant depression. All the patients in this trial had failed on at least two antidepressant drugs. They’d all failed on CBT. They were given a single 25 mg dose of psilocybin, and they all improved. A significant number, nearly half went into remission, and some of them are still in remission eight years later, although for the majority, the depression has crept back. But the effect size of psilocybin at one week and at three months is the biggest effect of a single dose treatment for resistant depression ever recorded in medicine. And it seems to me completely unacceptable that patients should be denied access to something like this when they have failed other conventional treatments.
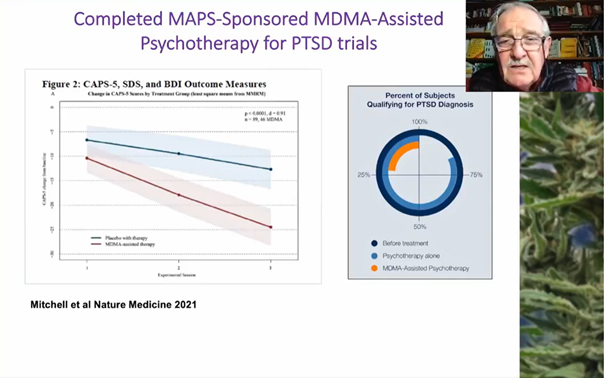
And then finally, here are the recent data from MDMA therapy for PTSD, post-traumatic stress disorder generated by the charity called MAPS. On the left hand side, you see the results of the first phase three multicenter trial of MDMA therapy, three sessions interspersed with about three months of weekly psychotherapy in terms of scores on CAPS, which is a standardised rating for PTSD symptoms. And you can see the red bar shows the much greater reduction in cap scores following MDMA during and following MDMA therapy compared with placebo. The significance level is 0.0001. The effect size is 0.91, which is a very large effect size. It was published in the leading journal Nature Medicine last year. And on the right hand side, you see a schematic of the impact of this intervention, comparing it with psychotherapy alone. And you see that following MDMA assisted psychotherapy, less than 25% of the patients still have the diagnosis of PTSD or is following psychotherapy alone, over 75% still may have a residual diagnosis of PTSD. So MDMA is offering a unique and powerful alternative an improvement for people who have failed on psychotherapy and also on conventional antidepressant treatments with PTSD.
I will finish now by saying that it’s been extremely difficult for the groups involved in this research to conduct it because of the scheduling of these compounds under the conventions. Very few countries allow research with these drugs. The fact it’s been able to be done, it should be celebrated, and we should now act on these findings and recommend that for research purposes, these drugs should be removed out of Schedule I. Very explicit indications should be made to all signature countries that research should be encouraged with these drugs because of the very powerful preliminary data I have presented today. Thank you very much.
Myrtle Clarke, MD at Fields of Green for ALL: Thank you very much, David. We will never stop in our quest to have your impeccable evidence heard. Our next speaker is Greek Zwele. Greek is a director at the Umzimvubu Farmers Support Network based in rural Pondoland, KwaZulu-Natal province in South Africa. We are grateful for Dr Zwele for his presentation today as he lives far from the nearest road and managed to contribute to our discussion today. Despite huge challenges with our intermittent electricity supply and unreliable internet signal in rural South Africa.
Cannabis has been used, cultivated and traded in southern Africa for over 700 years. The farmers of the Pondoland region have suffered years of aerial spraying of their cannabis crops using the known carcinogen glyphosate. Activists on the ground brought a stop to this inhumane practice in 2015, but any talk of restitution or compensation is not forthcoming. The Umzimvubu Farmers Support Network have made representations at the highest international level, but we have yet to see any meaningful engagement on the way forward for our traditional farmers and healers. When it comes to cannabis medicine – our colleague a true warrior for our beloved plant, Greek Zwele.
Greek Zwele, Umzimvubu Farmers Support Network, South Africa: My name is Greek Zwele, a traditional doctor and also a director of Umzimvubu Farmers Support Network which I’m representing here. We’re an organisation which stopped the spraying of cannabis in Pondoland. That spraying has been happening for more than ten years. Then after stopping it, the government changed so many laws in terms of cannabis. When they came up with the bill, we opposed the bill because it was restricting us to four plants and a maximum of eight plants per household, which we don’t want because this is a plant which has been used by generations and generations and for many things. It looks like we’re being denied to continue running our life the way our forefathers have been running and the way we’re running it now. We’re using cannabis for healing, medicinally, where people are using it for purging, cleansing, steaming and also making some medicines from it: for epilepsy, high blood pressure, many types of cancer, etc. We also use it to initiate the new Traditional Doctors and use it for when their spirit needs. We also use it for feeding animals, contraceptives, recreation, etc.
The government says it wants to replace our landrace with hemp, which we know it doesn’t have strength like our regional cannabis which is our landrace. We don’t want that. We would prefer that the government talk to us as growers and the people who are using this culturally. We also use it as an income generating commodity and it has helped us a lot. So many people educated and well off in Pondoland have used cannabis because it’s not only us as growers in the area who are using cannabis. There are so many people from this area who are using cannabis as it is a cultural plant and used strictly for good things. In Pondoland we don’t have cases which are not normal because of cannabis. We have been using the plant well-coordinated not disturbing any human beings. We therefore recommend to the government that at least each household should have a hectare of cannabis and government should assist us to have processing centres, to get good seeds economically, to grow the crop on large scale and to get market regulated by our government. All these bills they come up with are not community friendly, we don’t want them. Otherwise, they should start the whole thing from the beginning and consult with the communities. Do the right thing by the people. We are saying nothing about us or for us, without us. We have to be included in all the activities around cannabis. Thank you very much for inviting USFN to this very important meeting. I thank you.
Myrtle Clarke, MD at Fields of Green for ALL: Thank you, Greek, for that very moving presentation from your homestead in Pondoland. We certainly hear you and we will continue to strive to make the voices of the rural farmers heard.
Our next speaker is Mac Haddow from the American Kratom Association. The aim of the association is to support the needs of consumers and educate those involved in the use, sustainable cultivation and regulation of kratom, a plant that is an all-natural alternative in a world of increasingly dangerous pharmaceutical products. We are incredibly grateful to people like the Katom Association for educating us in civil society about sometimes little known plants. I know that in South Africa we don’t know much about kratom, so it is these civil society connections that are so valuable for our education too.
Mac Haddow, Senior Fellow on Public Policy, American Kratom Association: Hello, this is Mac Haddow, Senior Fellow on Public Policy with the American Kratom Association. I’m grateful for the invitation to participate in this side event hosted by Fields of Green for ALL here at the 65th Commission on Narcotic Drugs.
The AKA represents the 11 to 15 million American consumers, and we speak for millions of kratom consumers across the globe who would have been negatively impacted if the Expert Committee on Drug Dependence had concluded that kratom was eligible for either a critical review or for scheduling itself. We know that on December first of 2021, the ECDD voted in a conclusive 11 to 1 vote that there was insufficient evidence to justify any critical review or scheduling of kratom internationally. The reason is simple. Kratom has a long history of centuries of safe use in Southeast Asia and more recently, decades here in the United States. It is a question mark of significance as to how kratom was elevated to a prereview status at the UN Commission on Narcotic Drugs. And it raises fundamental questions about the current scheduling procedure at CND, given the long history of safe use of this plant. The conflict between kratom consumers and government officers was crystallised in the first repressive state sponsored ban in Thailand, beginning with the 1943 Kratom Act, and it continued for decades until those government officers finally recognised this mistake that they had made in criminalising kratom consumer use. In 2021, Thailand completed a years long process of correcting that mistake, and it should be instructive to every government entity because the science on kratom finally overcame the biased regulatory agenda of some member state government officials. The legalisation of freedom in Thailand ended a long record of misguided policies on a plant that has been used beneficially for the health and well-being and traditional rural communities and the residents in those areas.
The UNODC’s Global SMART Programme was initially set up to monitor illicit synthetic drugs, but somehow kratom was listed in the first major SMART report in 2011, where it was characterised as an amphetamine type substance. A plant that was supposed to be monitored as a synthetic drug finds its way into that report. In subsequent years, the SMART programme expanded its portfolio to characterise so-called new psychoactive substances to include, among other suspect products, kratom. This dramatic expansion of the definitions of what a new psychoactive substances is allows some member state government officials to reset the definitions and discussions on plant based products like kratom, simply because those government officials do not like kratom. We believe at the American Kratom Association that every decision should be based on science. We applaud the ECDD for their professional review that set aside the politics, and it demonstrated that biased kratom assessments made by some member state government officials is not a good replacement for evidence based scientific assessments of the safe, long term use of products like kratom and the benefits it provides to consumers. In 2016, the ECDD Working Group initiated some reforms that concluded that the “primary criteria for harm would be fatalities. In addition to other serious adverse events”. That was a welcome objective standard that took away some of the politics that were involved.
But it created the unintended consequence that some member state government officials then recharacterize their assessment of kratom and its so-called harmful effects. To claim that there were fatalities where kratom was present and they falsely asserted that kratom was in fact the cause of death. The United States Food and Drug Administration did it. 44 deaths, they claim, were caused by kratom. Those deaths became the political talking points, not scientifically valid death reports, but rather the politics in order to allow the FDA to make a claim that could then sustain an application under the U.S. Controlled Substances Act to schedule kratom, they were denied twice because of insufficient evidence. The science is clear. There are no cases in which kratom was deemed to have caused or significantly contributed to any of those deaths, and that was reported in the ECDD’s pre review report. The outcome, however, of the pre review of kratom was that it was initiated by an international organisation with supporting information regarding the fatalities due to kratom use is the problem. With regard to those fatalities, the U.S. reported that mitragynine, the constituent alkaloid of the kratom plant had been positively identified in 583 post-mortem cases between 2013 and 2020. And then interestingly, they claim that seven additional cases were reported from Canada and four European countries. Think about that from a statistical perspective. How is it that the United States had 583 post-mortem cases and these other candidate in other European countries had much fewer? Well, we know it’s because they reclassified in the United States what a kratom caused death was, and they didn’t do it according to science. They did it because of politics. Amongst all of those deaths, only two deaths, one in North America and one in Europe was identified, where kratom was the only substance involved. A subsequent analysis of a of a similar kind of report was made by the Centers for Disease Control in the United States, and they found after applying more rigorous analytical tools and more sophisticated equipment that even those were actually poly drug use.
The problem with kratom today is that there are cases where kratom is adulterated by a dangerous substance and that creates a health problem or a death. We know that’s true. It was true in 2009, which was the triggering event for the FDA’s interest in kratom when it was reported in Sweden that there were nine deaths in a twelve month period because of a kratom product called Krypton. A subsequent analysis by Swedish researchers found in a peer reviewed published article that, in fact, that the kratom product had been adulterated with a toxic dose of O-Desmethyltramadol. Same dose of that O-Desmethyltramadol in your cup of coffee in the morning or your glass of orange juice would kill you. It is not fair, and it is fundamentally not scientifically valid for anyone to make a claim about a death because of an adulterant that’s added to any product. And we think that’s a major problem with the analysis that was done and why there needs to be reforms in the ECDD process that would require any member state that makes an application for the scheduling of any substance to be able to document, with scientific rigour, the actual cause of death or the health problem that’s associated with any substance in the future. We advocate for that reform because we know that the threat of a ban on kratom that was initiated by these false reports and that was accepted by the UN Commission is the reform that’s critically needed.
We hope that in the end, science will rule the day, that in each case that we look at these substances and we measure and balance the health benefits that are provided, which kratom provides obviously. The Johns Hopkins University conclusively showed of adult kratom use that it helped people wean off of opioids. 35% within a year were able to wean off of opioids and go on to kratom. And we know in the opioid overdose crisis that we have in the world today that harm reduction should be the rule of the day. Thank you for this opportunity to participate in this side event and look forward to any questions that you might have. Thank you.
Myrtle Clarke, MD at Fields of Green for ALL: Thank you very much, Mac, and we certainly look forward to working with you in the future and unravelling these very complicated issues around the evidence of our beloved plants.
Our final speaker today is Brenda Perez from the Centro del Pueblo in Humboldt County, USA. The Centro del Pueblo is a community organisation that serves immigrant, indigenous populations in California with strong historical, social and cultural roots. The centre recognises the value of indigenous roots and offers a space for the empowerment of communities. Ms. Perez is an immigrant from Mexico, and her work includes fieldwork in areas of marijuana and coca leaf cultivation. She is the host of two bilingual radio programmes that highlight the importance of the immigrant community and the indigenous peoples of the South in the United States. We are honoured to have you with us today, Brenda Perez.
Brenda Perez, Executive Director of the Centro del Pueblo, Humboldt County, USA: Hello, my name is Brenda Perez, I am the executive director of Centro del Pueblo in Humboldt County, California, United States. We find ourselves in a period of transformation and opportunities to exit the labyrinth of violence caused by the war on drugs. The reforms in the drug policies from Uruguay and Bolivia to Canada and the US is leading the path to correct a historical mistake of scheduling the coca leaf in the list one as a dangerous drug, ordering its eradication. By recommending a rescheduling of the coca leaf, international agencies could allow us to clarify different dynamics that pursue new
forms of development, equity, security and justice. It comes a time for a review based on evidence to regulate the potent markets of these millinery plants beyond borders. It is a time to look at the research that includes extensive fieldwork with a close approach to the most affected people and to the actions of the new generation that keeps protecting the use of coca as their ancestors did. Some highlighting research based on fieldwork make us hopeful about the future – First, the alternatives for controlling the extension of coca cultivation, the focus on environmental protection and social development, and also the potential of revitalising the traditional coca market with the case of Argentina and Bolivia.
The story of coca – The coca plant is a symbol of cultural diversity with deep social roots. It is an element that articulates ceremonial, medicinal and political dynamics through local and international history. Archaeological evidence has shown that Indian societies were already chewing coca leaves 1000 years ago, in addition to being a basic trade product since ancient times. After millennia of the use of coca, we can observe the violent effect of prohibition in the recent decades due to a policy based on a misunderstanding in the traditional use of the coca leaf and the denial of the many benefits to human health. The resulting legal ambiguity is obvious since countries have a dual obligation to prohibit and abolish the chewing of the coca leaf and at the same time to implement measures that respect human rights and the traditional licit consumption. So what are the alternatives for controlling the extension of coca cultivation in case of rescheduling? These alternatives are already ongoing in Bolivia and Peru, where there has been a determination amongst the community to keep a system of rationalisation. It’s an agreement to eradicate certain areas allowing for land restoration and to self-regulate the crops.
Decision making process – The coca growers community discussed in a very vibrant way, the system of social control over production referring to community self-control to prevent illicit activities around the coca leaf. The traditional system of collaboration sustains this model of sharing profits. They also proposed regulation of a foreign trade model, for example, in the border with Argentina. This is an area of opportunity. Rescheduling of the coca leaf will encourage the production of knowledge about these initiatives through the creation of research centres in the production area. And these could increase sustainable production for generations. Another possibility is to acknowledge the potential of coca in therapeutic uses as a detoxifier agent to substitute the use of cocaine. These experimental tests are being carried out in La Paz, Bolivia, where a group of experts perform this therapeutic use.
Coca beyond borders – It is necessary to recognise the areas of opportunity to broaden the influence of the coca market with official recognition of the inter-American coca trade route between several countries such as Colombia, Ecuador, Peru, Argentina, Chile, Bolivia, Paraguay, Brazil and so much more, which dates to the 16th century. Let’s focus Argentina market for example. Since 1999, Argentina legislation protects the possession and consumption of coca leaves in their natural state. However, given the lack of cultivation in the country, ambiguity arises about the supplies of the leaf giving way to a great area of commerce with payment of informal taxes. This specialised market is very vibrant. The coca leaves have become one of the most interesting products in terms of its diversity in the local markets. They life is offered as “come on, select”. It has to do with texture and size. They are also offered with a seal of origin from large jungles in Bolivia for the most privilege of consumers. The area of opportunity here is to investigate the potential of the Argentina coca leaf market and its consumers through the elaboration of a census.
What is going on in the region and what will be the next step in the regional agenda? To promote forums and festivals of the coca leaf. To publicise the benefits on health and to promote organic production. To promote higher education, the research of the coca leaf and to promote ancestor culture in basic education. To promote the application of a study of consumers to another dimension of the market in different countries. Support exchanges between traditional coca leaf producers about the ecological sustainable growing techniques, this ancient knowledge that needs to be recognised. Finally, the creation of a trade agreement at the regional level who set the tone for achieving a model of regulation once the coca leaf is rescheduled. The future is now. Reschedule coca leaf. Thank you very much.
Myrtle Clarke, MD at Fields of Green for ALL: Thank you so much, Brenda, so many common issues across the board when it comes to our plants and so many hardships experienced by the producers of the prohibited plants across the globe. We also look forward to working more closely with your organisation on these very common issues.
Civil society works very hard to bring evidence and solutions to the worldwide policy issues in order to protect all of our human rights. I would like to draw attention to a recently published paper by our colleagues, Kenzi Riboulet Zemouli and Michael Krawitz, from FAAAT think & do tank. This paper is entitled High compliance, a lex lata legalization for the non-medical cannabis industry: How to regulate recreational cannabis in accordance with the Single Convention on Narcotic Drugs. For those countries around the world and their governments who are considering unleashing these plants for the use and benefit of their citizens, we strongly recommend that you, as activists who are watching and people with the say and who are heard in their various countries, pay attention to this paper.
I’d also like to draw your attention to Fields of Green for ALL’s very own manifesto that we are incredibly proud of. Published on the 20th of April 2021 and entitled Cannabis in South Africa: The People’s Plant. A Full Spectrum Manifesto for Policy Reform. As Greek was saying earlier, nothing about us without us. And we also know that you can’t get what you want unless you know what you want. So we know what we want, and that is why we have published this manifesto and it is available for download from the Fields of Green for ALL website. Please visit Fields of Green for All website for any information that you require.
In conclusion, I would like to leave you with one example of the harms of unscientific evidence and moral drug judgements in drug policy. Over the last eleven years, we have heard it stated on numerous occasions, most notably within our South African Parliament two weeks ago, that cannabis leads to risky behaviour and therefore increases the risk of HIV transmission. This has never been scientifically validated. And given the enormous resources that have been dedicated to fighting the scourge of HIV aids and communicable diseases worldwide, it is exactly this kind of misinformation that needs to be stopped. It is disrespectful to all the people around the world who are fighting the various challenges that we have on our planet across the board. In the words of our Macedonian civil society colleagues, ladies and gentlemen, good people disobey bad laws. And with that thought, I would like to leave you and thank you for joining us today.