Opened by Chair of CND, Amb. Srisamoot.
Amb. Srisamoot. Thanked Amb. Hansen (Norway) and Amb. Stewart (Australia) for convening the panel. Other specialized agencies from UNODC, WHO and civil society. CND has had numerous sessions where we have talked about availability of controlled medicines and this event serves to reinforce and highlight the importance of the issue. Access to controlled medicines is a critical topic for the commission in its preparation for UNGASS 2016.
Amb. Shamaa Chair of UNGASS board. Wished everyone a happy Eid. Agrees that availability is an important topic for UNGASS. Lack of availability in developing countries is a major health problem, which must be addressed together. Quotes SC for relief of pain and suffering and foresees that adequate provision must be made. JMS adopted highlighted need for MS , INCB, and UNODC in cooperation to address the situation by taking measures to ensure that availability was made, while simultaneously preventing trafficking, etc. Ensuring availability also the center of one of the interactive discussions in March, and will be pending a resolution to be discussed in roundtables during the special session. Notes that today’s event is a very important discussion on this issue. Hands over to Amb. Hansen.
Amb. Hansen: Perm. Representative of Norway. Echoes warm words of welcome. Particularly pleased to have so many distinguished colleagues from WHO, as often sees the need to coordinate work with them. Also a pleasure to co-host with distinguished Australian colleague. Some topics permit a passionate response, and this is one Hansen is passionate about. There are divisive issues when it comes to UNGASS, and continued discussion among member states and other countries alike is required to develop a good policy response. But the topic of this meeting, TOPIC read, should NOT be controversial. It should unite us all across regions and national borders. Last week we attended general congress of IAEA and adopted an important resolution on cancer therapy as cancer is now the leading cause of death worldwide, having surpassed cardiovascular diseases. Millions of people are waiting to see what UNGASS will do with respect to essential medicines. We want a very clear message about access to essential medicines for maximum impact and we must not disappoint those who depend on the outcome. This is a humanitarian issue of the utmost importance. Indeed it is a human right. For all of us who have experienced cancer in the family or with close friends, we cannot but agree. In many countries access low or non-existent. We need to close these gaps. We need to have national regulative framework and then make medicines affordable through the private sector. UNGASS creates an opportunity to make world drug policy more human and fair. We must make full use of it. Objective of conventions is to advance health and welfare of mankind. Nothing Less, Nothing More.
Amb. Stewart. Australia has had a long standing commitment to working to address this problem. Stewart’s job is translating concerns of many countries into effective action. Refers to a global distortion in problems faced with controlled substances, painkillers, etc. In some countries there is abundant availability. In a few countries there are problems of abuse, but in most there is a serious lack and sometimes no availability that most of the world takes for granted. One of the great achievement of the UN in this area was to create control system, but we need to recognize that there is a problem and it has not worked as intended. Barriers to access exist, but to be resolved they do not require large monetary commitments through international programs. Rather they require organisation, technical assistance, and above all partnership. I am delighted that a number of distinguished colleagues from WHO have traveled to Vienna to do this. What is needed is increased cooperation between major players and MS. MS views this as something we need to work together on in order to make progress. Initial contributor to joint global program. First part held in Ghana. We support the work of WHO in looking at how to improve policy and we very much hope that others will join us. Expresses need to establish a permanent program.
Amb. Hansen Complements Australia for actually doing it, and working in country.
Kees de Joncheere (WHO) Access to essential medicines one of the six priorities of WHO under Director General Dr. Margaret Chan. Goes through different resolutions of WHO on access to essential medicine. Notable that China has one. Describes WHA resolutions on pain and palliative care, essential surgery and anesthesia. Estimates that only 15% of people who need palliative care actually receive it. WHO is one of the partners to SC and has a specific mandate – it is not just about preventing drug abuse, but ensuring access. Very important issue for global public health. Three streams of work involved here — Dept. of essential medicines, work with ECDD and mental health and prevention and treatment of drug disorders. Details global action plan on NCDs and area of HIV AIDS and other blood borne diseases. Suggests a strong public health approach through harm reduction is required. UNGASS will be on upcoming agenda of EB in January and will also go to WHA and this whows importance to colleagues in Geneva.
Amb. Hansen We are so happy to have Chair of UNGASS board and CND here. Testimony to the work continuing.
Dr. Gilles Forte. WHO Coordinator for policy, access, and use of health products. Leads secretariat of EM and ECDD. Refers to slides. Huge attitude problem among providers. WHO added specific medicines for pain on the model list. About 12 medicines that are controlled are considered essential medicines. Have unique efficacy and safety profile. Should be available in health centers. WHO has also recently developed a number of treatment guidelines to identify treatment of choice for children, and for opioid dependence. Guidelines for pain in adults are in the making. Secretariat is assisting in compiling guidelines and national lists to ensure that the controlled meds for pain are included. Collaborating with MS to make medicines more affordable and to ensure that governance of the pharmaceutical sector is improved.
There is still a huge need to strengthen capacity of professionals. Engaged in about 40 countries. Around 20 of these in Africa. WHO Secretariat works very closely with partners, Civil Society, INCB, UNODC to achieve aims. Recently completed ATOME in Europe. WHO part of joint global program with UNODC to improve access in Ghana. We have also worked together with INCB to develop guide for improving quantification for medicines and we know that we need to do more to make sure that countries use this guide more consistently. Currently working with UNODC to develop model law. And finally engaged in a number of countries in Africa and AU to carry out a series of workshops to strengthen capacity of professionals in prescribing and using CM. We see this meeting and all the work we have started with partners as an opportunity to contribute more strongly and forcefully to the UNGASS agenda and to make sure that the issue is really elevated in those discussions. We are very keen to discuss how to scale up this collaboration with our partners.
Dr. Gilberto Gerra. Starts with a word that Amb. Hansen used. “Passion” — we have to be engaged with passion when we speak of people with no voice and those affected by other suffering such as dependence, HIV, etc. The health aspects of our work should all be treated with passion, and not as a bureaucratic issue. We should disregard a “prohibitionistic regime”. Preamble of SC says purpose is to guarantee access to indispensable medicines for the relief of suffering. The International community is still not taking concrete action. Should not discuss as a philosophical debate. These drugs are on the street but not in hospitals or pharmacies. They are sometimes counterfeit and dangerous, but they are still there. Protecting the health of people from the dangerous effects of drugs is not in conflict with guaranteeing access to essential medicine. The international community is in danger of double failure, being both unable to stop abuse, and provide access. Emphasized need for morphine. Then notes other controlled medications for epilepsy, etc. Describes history of legal use of cocaine as a local anesthetic and in reducing bleeding, as well as applications in surgery.
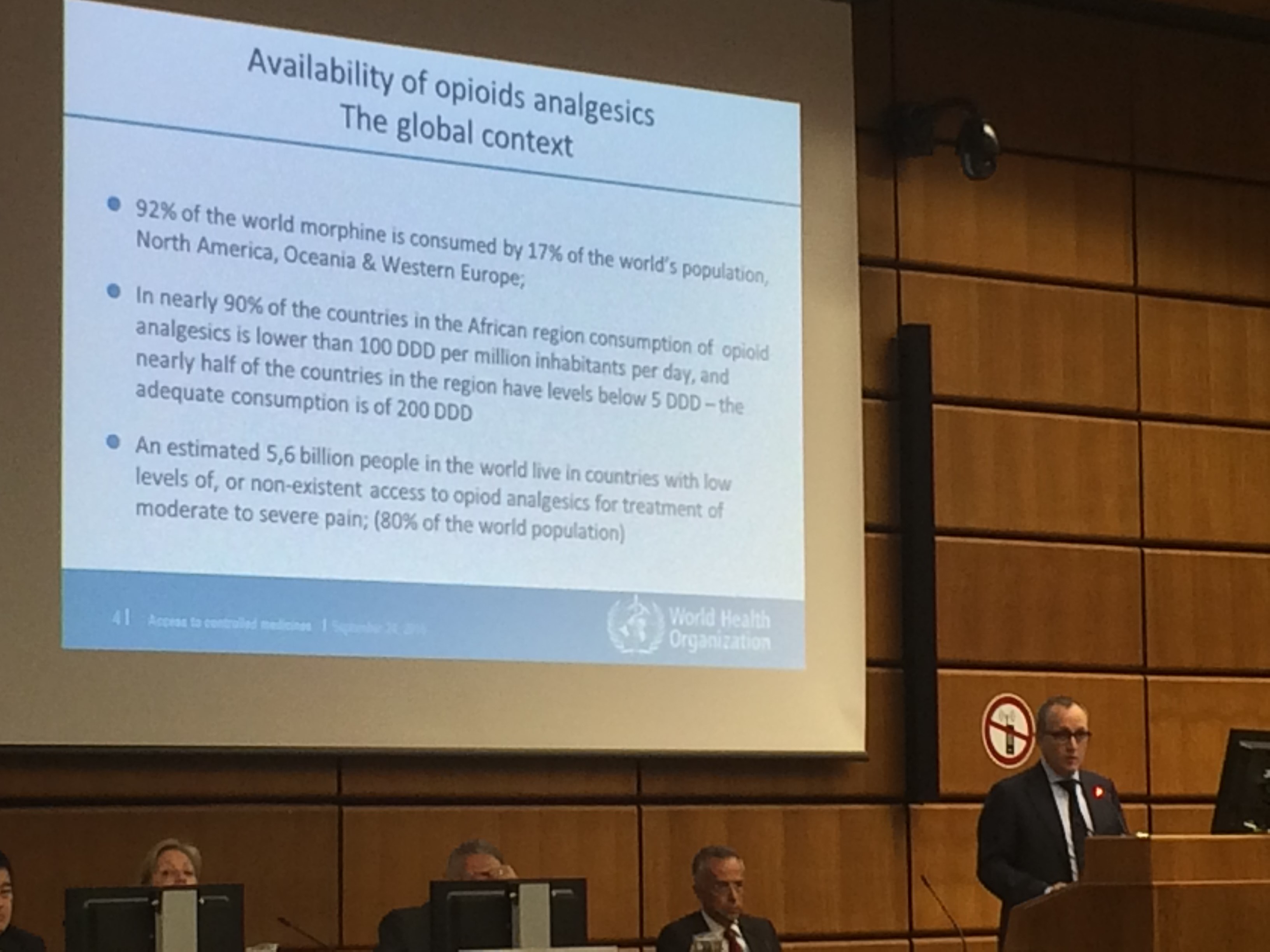
Ketamine. Reasonable decision of MS not to put ketamine under international control and reasonable decision of China to withdraw. When a drug is put under control, it becomes less available or unavailable in low income countries. Drug control system has to change mode of controlling these drugs as part of highest attainable standard of health. Notes a disparity in global consumption statistics with large gaps for some countries. Notes that availability is not related to abuse. Some instances show high availability and low abuse, and then high abuse with low availability. Refers to slide. Have done an exercise looking at 2010 document with INCB asking: What are the reasonable provisions of the conventions? Trying to remove barriers. Preparing a new generation of health professionals, policy makers law makers. To avoid diversion and misuse of appropriate rules and conventions.
Iatrogenic epidemic of prescription drug abuse in the US. Important to have correct assessment of person before prescribing. Have to evaluate characteristics for risk of persons. Use medication in strong relationship with patient. It is important to have Interpersonal relations of compassion and support. Acknowledges that there is a fear of dependence. Many don’t understand that becoming physically dependent doesn’t equate to addiction — this involves exposure of brain to medication plus genes and other vulnerabilities. Looking again to Africa, because of pollution and changes in lifestyle there has been a huge increase in cancer. 1 million per year by 2030 because of lack of infrastructure and diagnostic opportunities. Most will be diagnosed in last stages with metastases. Full respect for individual attitude, must stop ideological approach. Giving pain medicine is materialistic…spiritual and religious. Leave science out of this debate. Suffering of another human being is my suffering.
Dr. Saxena WHO Substance abuse psychiatrist. Director for Mental Health and Substance Abuse at WHO. Explains that this event has been called a side event or special event. This is one of the central events for those of us who feel very passionately about it. So far we have heard about access to medicines. But what other aspects are important and which ways are WHO preparing MS for more informed discussion for UNGASS? When we say WHO we mean MS and the Secretariat. We are very much listening to MS. Why is public health approach needed for World Drug Problem? Refers to slide. MS are now clearly asking for a strengthened PH approach. There are four important resolutions for WHO mandate. Last time WHO discussed drug policy was during 1990 resolution in assembly for demand reduction. On the request of MS, bureau has accepted to include UNGASS and world drug problem as an agenda item in January 2016. This will help us hear views of MS more clearly and present our best approach in preparation for UNGASS.
JMS has very clearly pointed out a focus on these issues. These are milestones for drug problem in UN systems. There is the Human Rights Council 30th Session coming on Monday as well as many UNGASS meetings, formal and informal. There are three important roles, mandates and activities of WHO. Prevention of drug use and treatment of drug use disorders, treatment of blood borne disorders, and improved access to controlled medicines. Slide shows estimates of deaths due to drug use disorders increased in last few years. Burden attributable to drug use being especially high for young people. Treatment and HIV prevention and coverage are low. Access to other health services also very low all over the world.
The Pakistan Framework of drug control conventions can help with this staggering problem. Medical will seems to be increasing. UNGASS can use this reservoir of political will to address the problem.
Amb. of Mexico. Congratulates initiative. Useful for the debate and useful for the Mexican delegation to get updated on information about WHO, as well as making connections with HRC. It is critical. Asks whether panelists could go one step further to tell us what needs to be done. Acknowledges that WHO is working on the issue and happy that they have put item on the agenda, but would like to hear recommendations from WHO to member states before meeting in Geneva so that Mexico and others can somehow influence development and outcome of the session. Mexico calls for action and recommendations. Would like to see more interaction between WHO and member states and not just information sharing. Notes some things that Mexico could have been doing differently to improve the problem of access. This is a huge violation of human rights if we look into the suffering of so many people in the world because of issues like bad regulation and lack of training.
Slovakia. Is there not a huge barrier for low and middle income countries because of prices?
Australia. Can support the current program. Doesn’t support large amounts of funding. With three or four pilots, this could get to critical mass. Could get to something that delivers effective results and builds partnerships that are evidently needed.
Netherlands. We know the barriers but not much is happening. We can create a bit of momentum and political will to address the issue increasing. Refers to subject of resolution INCB electronic system. Still a physical paper trail to export from Netherlands. Should do so by email and not physical mail. INCB has a system, but needs more funding. To do this, copy and paste in UNGASS outcome document followed by recommendations.
Kees de Joncheerse, WHO. Agrees cooperation is needed. Doing things together is the reason we are sitting here. Need a collaborative program. Also wants to step-up efforts. Small start but with your support we can intensify that. On the issue of prices, in fact most of the medicines are off patent and so are generic and don’t cost much to make. We have made the market so difficult for the private sector that manufacturers are not interested in producing. The current way we manage the market drives prices up. This is not just evident with controlled meds but other generics. In controlled medicines we have created the system that confuses the markets.
Dr. Saxena. Recognizes need to work more closely. In response to Amb. Mexico, says we do need to interact more and need to step up efforts. Promises this will happen.
Dr. Gerra. Financial aspect always important. No difference between buying ketamine and morphine. Resources are being put to use in wrong direction, but could be reorganized in a positive direction. In response to Amb. Mexico, we must form a partnership — tripartite. Must test cooperation in the field. Must work with policy makers to change their mentality. And to train professionals and influence public opinion. Patients often not ready for some medications. Atomic agencies want to be on board. They are taking care of people from radiotherapy point of view.
Amb. Hansen Thanks everyone. Brings to a close.