
Organized by the Medecins du monde with the support of Australia, the Netherlands, and the International Network of People who Use Drugs, the UNAIDS and the UNODC HIV/AIDS Section
The new Global AIDS Strategy and 2021 Political Declaration on HIV and AIDS include bold new targets on ‘social enablers’ and community involvement which can be utilised by Member States to inform better approaches to drug policies. Join us for a discussion breaking down these targets, their relevance to drug policy, and the central role people who use drugs have in both the global AIDS response and building better approaches to drug policy.
Chair: Jake Agliata, Policy and Communications Officer, INPUD
Thank you for joining our side events – thank you particularly to our co-sponsors. Housekeeping rules – we are recording. Interpretation available in Spanish, French and Russian.
Opening Remarks: Judy Chang, Executive Director, INPUD
Welcome everyone. INPUD has always been very tied to HIV movement. Health inequalities aren’t natural phenomena – the war on drugs pushes people to the margins. Lack of funding for people who use drugs and peer-led programs. Global HIV response (10-10-10) and 2030 targets need to be brought to bear on drug policies. Particularly today – INPUD stand with people who use drugs in Ukraine. We have a guest speaker here today representing people who use drugs in Ukraine.
Galina: I speak on the behalf of people who use drugs in Ukraine and Ukrainian Women who use drugs.
I can’t say everyone is safe now. I will convey their positions. Any crisis always shows the most vulnerable spots of any system. For many years, the Ukrainian Network of People Who Use Drugs has been building sustainable HIV programs, working to ensure equal access to reduce stigma and discrimination. This horrible crisis has shown we have not done enough. We work together to influence public policies and for gender sensitive services. If it weren’t for the war, we would be talking about our achievements. But the criminalisation of people who use drugs is one of the biggest obstacle of safe movement in the region – scared that they wont receive OST or ARV services. In the occupied territories, OST programs are closed. Pharmacies cannot sell controlled drugs or are closed and cannot provide services. Moreover we have observe the growth of stigma and discrimination against people who use drugs – COVID was the first sign of this. We urge everyone working on the HIV response, that without solutions people will be in danger, and crisis will kill them. Let’s show by action.
Suki Beavers, Director, Gender Equality, Human Rights and Community Engagement, UNAIDS
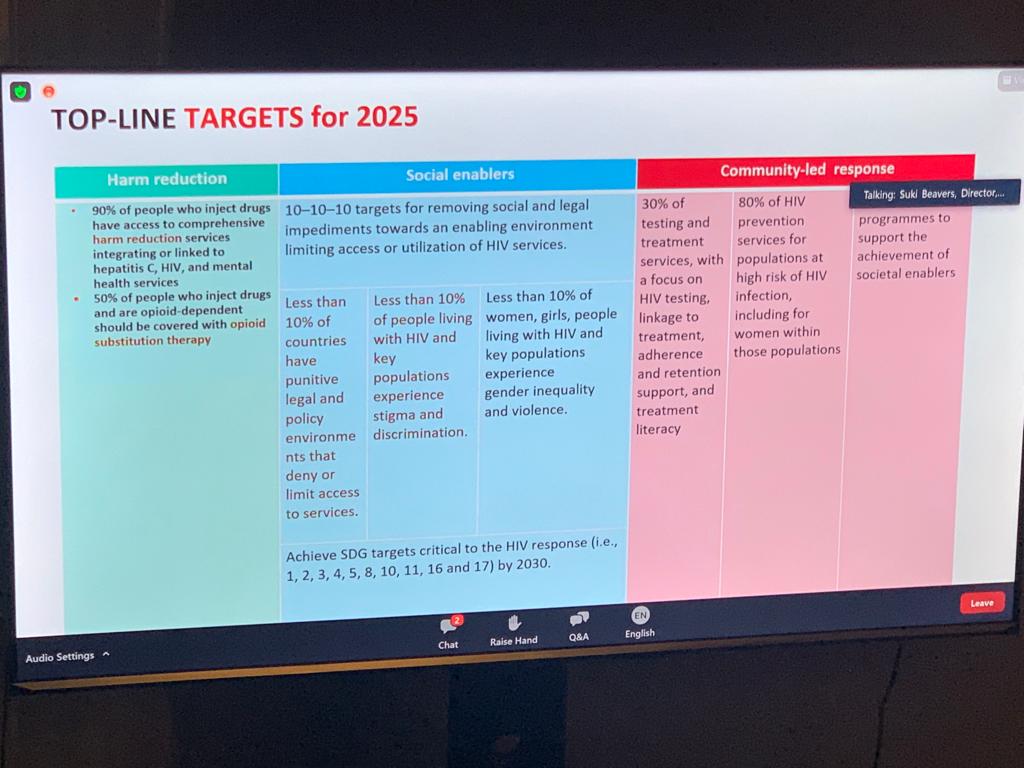
Millions of people who use drugs are left behind in global AIDS response. Decline in global new AIDS infection between 2010-2019, but there is no change in incidence in people who use drugs (some regions have increased). Full targets are supposed to be reached by 2025. Low access to services among people who use drugs is one of the biggest gaps. The new Global AIDS Strategy promotes access to harm reduction programs and OST (we are so far behind) – 90% people who inject drugs should have access to harm reduction services.
The UN Common Position committed to moving towards decriminalisation – only 23 countries allow for progress on decriminalisation. UNAIDS committed to community led service delivery – by community led, we mean peer-led, because we know that this works. People who use drugs are instrumental in these responses, and need to be recognised as experts and empowered to lead.

 We can’t reach targets if drug use is criminalised, and if people who use drugs don’t lead programs. A platform we use to intensify efforts towards these targets is the Global Partnership for Action to Eliminate all forms of HIV related S&D, to inspire these countries. 29 countries have joined in past year. We have developed guidance and tools for this, to reduce drug-related stigma. I want to express support for people who use drugs in Ukraine – we know that you are facing life threatening circumstances and need access to harm reduction services – UNAIDS calls on all partners to provide access to harm reduction in these times.
We can’t reach targets if drug use is criminalised, and if people who use drugs don’t lead programs. A platform we use to intensify efforts towards these targets is the Global Partnership for Action to Eliminate all forms of HIV related S&D, to inspire these countries. 29 countries have joined in past year. We have developed guidance and tools for this, to reduce drug-related stigma. I want to express support for people who use drugs in Ukraine – we know that you are facing life threatening circumstances and need access to harm reduction services – UNAIDS calls on all partners to provide access to harm reduction in these times.
Aditia Taslim, Advocacy Officer, INPUD
I’m here to talk about how the targets are being used on the ground. I’d like to extend my appreciation to Galina. First time in history of global politics of HIV that decriminalisation was supported in the political declaration. 2018 – three year process of consultation – led to 10-10-10 and 80-60-30 targets. Key populations and community led responses are also mentioned in these strategise – we demand no more lip service. We conducted a global consultation of people who use drugs and INPUD was part of negotiations of Political Declaration – this has not been without pushback. Some member states push backed mention of people who use drugs. Human rights and harm reduction are needed to reach commitments by 2030. Without pushing for accountability, none of the targets will be met. Pathologisation of drug use – systems are designed for diverse populations of people who use drugs. To achieve global targets, resources must be directed to key populations. Programs must be provided and monitored by people who use drugs. INPUD has published technical briefs on the 2021 Political Declaration and translated them into actions on the ground to provide action on the ground.
Growing political conservativism – we call for governments, UN agencies, and donors to recognise people who use drugs as valuable and fundamental in programs.
Today we call for full protection of rights of people in hostile environments in any part so f the world whose rights are violated. Stand in solidarity with our brothers and sisters in hostile environments in Afghanistan and Ukraine.
Fariba Soltani, Chief, UNODC HIV/AIDS Section
Thank you to all previous speaker – my comments are in line with yours. Thanks Galina for your bravery – we stand in solidarity with you, and with our colleagues and people who use drugs in Afghanistan. Continue services of people who use drugs and people in prison as much as we can. 65% of all new infections globally are among key populations – PWID 35 times greater risks than those who don’t exist. HIV infection in prisons is 4.3% – 6 times higher than adults in general population.
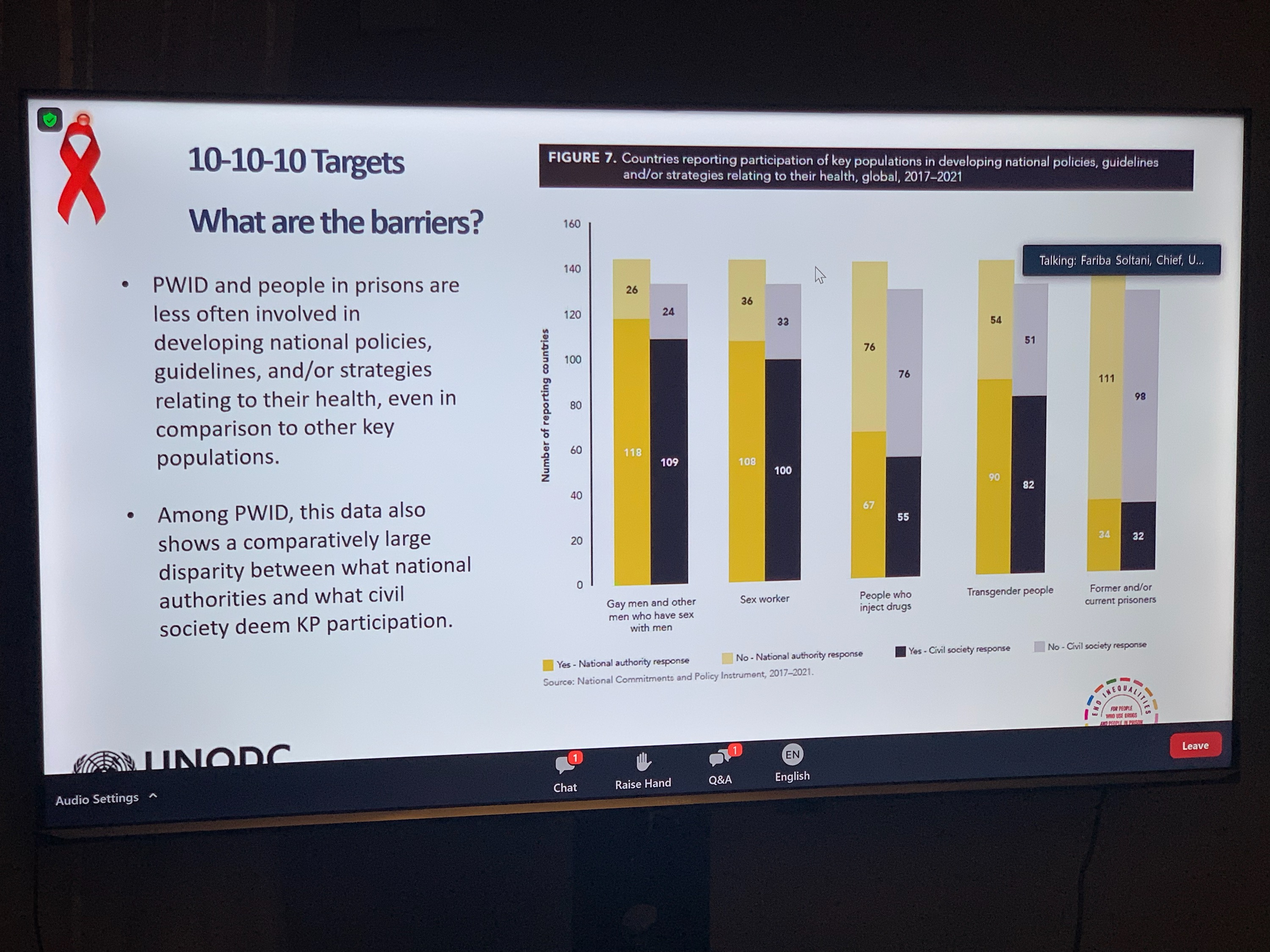
Global AIDS strategy and UNODC strategy – we working to make these strategies work in synergy. UNODC strategy calls for MS to scale up access to service, especially among vulnerable populations. We also have targets for community led interventions. Barriers to 10-10-10 targets – World AIDS day report – people who inject drugs and people in prisons are not involved in creating guidelines and strategies compared to other key populations.
Legal Environment – many countries continue to use discriminatory policies – this has been shown to block access to services and increase HIV risk.
There is growing political commitment to these issues in the following strategies:
- UNGASS 2016 Document
- 2019 Ministerial Declaration
- UNODC Strategy 2021-2025
- Global AIDS Strategy
- High Level Political Declaration on HIV 2021
We are coordinating webinars on implementing harm reduction in Africa – this shows the commitment of countries to ensure harm reduction services are expanding. Also the approval of implementation of OAT in Egypt has been great progress – a big achievement after many years of advocacy. Vietnam also implemented take home OAT in 2020.
We are bringing law enforcement partners on board – to ensure all stakeholders are around the table in terms of removal of legal barriers and discriminatory laws. We want to strengthen partnerships between health, criminal justice, law enforcement, prison administration and civil society – we have trained over 5000 law enforcement officers and brought law enforcement and civil society together.
In relation to prisons, we are promoting non-custodial alternatives to incarceration for minor, non-violent offences; we recommend reducing incarceration of PWUD and to end the use of compulsory rehabilitation.
10-10-10 targets
- UN Common Position on Drugs – the lead of the task team
- UN System Common Position on Incarceration – working to reduce incarceration
Millions within key populations remains invisible – we need to have better data and evidence – the total number of female sex workers, men who have sex with men, people who inject drugs and transwomen is probably double the current size estimates.
UNODC fully supports the implementation of the 80-60-30 targets, which include:
- Scale up of community led service delivery for PWID
- Integration of PWUD community led HIV responses into all national HIV responses
- Adequate resources allocation for sustainable community-led responses
Pascalle Grotenhuis, Director of Social Development & Ambassador for Women’s Rights and Gender Equity, The Netherlands
Thank you Galina for your story, I’d like to echo comments – we stand with solidarity with you.
This topic is close to my heart – how to share policies and programs – people should be at the centre. The system should work for the people, and not the other way around. We can’t end HIV epidemic or world drug problem if we don’t listen to the people. We need to empower people who are scared to access services. The Political Declaration on HIVAIDS and the new global AIDS strategy – less than 10% of countries have policies that reduce stigma and eliminate gender based violence.
Removing legal and structural barriers, people who use drugs need care they don’t need blame. Understanding their views should be our main priority. Stigmatisation needs to be reduced. I will echo SANPUDs messaging from a recent event: when providing HIV services, there should be no expectation of abstinence. Harms are largely due to prohibition. Netherlands supports this – community-first means putting people before the problem (drugs). We want to enhance people to advocate for their own rights. We look forward to working with you to reach these targets.
Aniedi Akpan, Executive Director, Drug Harm Reduction Advocacy, Nigeria
Stigma, discrimination and criminalisation of PWUD and achievement of the 10-10-10- targets
Attitude generally is still very discriminatory – to test people for drug use before providing treatment. We have stigma from the government, also discrimination, criminalisation, exclusion of people who use drugs in decision making.
Drug law enforcement agency – someone was arrested for 0.04kg (4 grams) of cannabis – this represents who this is being treated in our countries.
Effects on HIV services for people who use drugs in Nigeria include: self-stigma, loss of self-esteem, lack of desire to access services, increased risk of HIV due to incarceration, lack of government funding, lack of people who use drug-friendly services, resistance to rollout of evidence based harm reduction services, inadequate geographic reach of donor-funded interventions, lack of evidence-based and qualitative data to inform programming, lack of community structures for community based HIV prevent – because of criminalisation, lack of representation on decision making bodies
Our calls to action include:
- Address the tripartite barriers of stigma, discrimination and criminalisation by individuals and states to enhance investing in the drug user programming
- Include people who use drugs in planning and monitoring of HIV programs
- Need to expand community-led services for people who use drugs to cover geographic space
- Need to integrate people who inject drug-friendly services into public health facilities
Angela Wallbank, Australian Department of Health
The Global AIDS epidemic remains an important issue for Australia and will continue to actively contribute to the response, including taking steps towards achieving target 3.3. of the SDGs which seeks to end the AIDS epidemic by 2030. While the 2019 Ministerial Declaration noted with concern that the transmission of HIV associated with drugs remained high, it committed member states to ensuring that no one affected by the drug situation was left behind. We acknowledge the impact that COVID-19 has had on joint commitments to address and counter all aspects of the world drug situation and remain aware that those who are affected by the world drug situation, particularly key populations, are being disproportionately affected by the pandemic.
As part of the COVID-19 health response, and in efforts to mitigate the pandemic’s drug related consequences, Member States should continue to be mindful of these key populations. In 2021, Australia proudly worked with Namibia to co-facilitate the Political Declaration on HIV/AIDS at the UN General Assembly High Level Meeting on HIV/AIDS. The declaration was ambitious – putting human rights and addressing inequalities at the centre of the HIV response, and includes Member States’ commitments to put the global response back on track. As part of this PD, MS committed to urgent and transformative action, including to end the inequalities restrictive and discriminatory laws, stigma, and multiple and intersecting forms of discrimination that perpetuate the global AIDS epidemic. Australia was particularly encouraged by the inclusion and retention of text highlighting specific concerns with the low local uptake of harm reduction programs, and the persistent stigma towards, discrimination against, and marginalisation of people who use and inject drugs. Australia also welcomed the Declaration’s strong emphasis on people who inject drugs as a key population requiring tailored HIV prevention approaches and commitment to prioritising accessible, appropriate, person-centred services that meet diverse and multi-faceted needs.
Domestically, Australia’s 8th National HIV Strategy sets the direction for Australia’s continued response to HIV, and identifies people who inject drugs as a priority population. Similarly, Australia’s National Drug Strategy also promotes reducing risk-taking behaviours through public policy and programs to reduce harm. Both strategies champion harm reduction approaches to addressing drug use, and prevent the transmission of HIV, including through the implementation of needle and syringe programs, alcohol and other drug treatment and support programs, and measures to address social determinants of health. Central to harm reduction measures and approaches should be the involvement of people living with HIV, and those who inject and use drugs, to ensure that policies and programs are appropriately tailored and community-driven.
The 2016 UNGASS Outcome Document specifically reaffirmed the need to strengthen cooperation between UNODC and other UN entities when implementing the drug control treaties and intensify the meaningful participation of, and support and training for, civil society organisations and entities. Internationally, more still needs to be done to facilitate this involvement if progress is to be sustained, and ambitious global targets are to be achieved. We welcome and embrace the opportunities for stronger collaboration with civil society, particularly peer- and community-led organisations to drive evidence-based debate and multisectoral action forward at CND65 and beyond, and through the broader UN system. As Australia reaffirms it’s commitment to the international drug control conventions, and towards accelerating action towards the attainment of the SDGs, we also commit the supporting and advocating for the rights of key populations to be involved in the development and implementation of policies and programs that affect their community.