Item 5 (d). International cooperation to ensure the availability of narcotic drugs and psychotropic substances for medical and scientific purposes while preventing their diversion
CHAIR: Introduction to Item 5d. We offer the framework to scale and improve the availability of narcotic drugs and psychotropic substances for medical and scientific purposes. This issue is very important to my home country, and to all of us.
UNODC: Introduction to Item 5d.
WHO: As part of our mission of providing healthcare worldwide, we are committed to improving access to much needed medications, especially in the wake of the Covid 19 pandemic. Disruptions to the supply chain have effected health worldwide. Urgent action is needed, especially for those in emergency settings. WHO released guidelines for national policy regarding safe use of controlled medicines. We strive for policy that increases access to medicine, but prevents abuse.
International Narcotics Control Board: Many medications are consumed by high income countries. Lack of availability needs to be addressed. Emergency situations remind us how essential these substances are for the wellbeing of patients. We implement our learning project to help governments address controlled substances. There has been progress since 2016 in learning about how to best handle controlled substances.
European Union: We condemn Russia. We share concern of INDCP over Ukraine and access to medicine. In emergencies, it should it be allowed to quickly and efficiently provide medicine. The EU action plan addresses this issue. It also updates our view on controlled substances and pain relief. During our last session, difficulties experienced by member states were expressed. Despite efforts, progress in this area is not sufficient. We continue to deny relief to patients in serious pain. We see importance of continued international cooperation, data collection, and analysis.
China: All controlled substances have been scheduled in China and we continue to add more. We have stepped up drug control efforts. We make timely choices on drug manufacturing to keep up with demand. We encourage pharma companies to take supply chain issues into account for production.
Thailand: We recognize importance of this issue. There is an increasing need for medical drugs in Thailand for pain and palliative care. We support using an early warning system, monitoring systems, and facility inspections.
Spain: We agree with statement by EU. In Spain, we promoted various ways to avoid shortages, including logistical support and speeding up import processes. Medicine plays in essential role in public health. We have a challenges of providing medicine while making sure there is no diversion. We should learn from the experiences of other countries’ existing regulatory systems.
Russian Federation: Technical problems
India: To address these challenges, India has used a reponse that is based pimrarily on the criteria of healthcare, and preventing the infection among patients and health providers. Many patients receiving this treatment used to visit the service providers everyday to receive their medicine, such as buprenorphine or methadone. This is directly observed as we know you cannot control medications under the existing international conventions as well as under the Indian laws and regulations and hence procuring dispensing these medicines is subject to varying degrees of regulations, although we need to minimize the risk of their divergent presence. However, the extraordinary situation in the form of pandemic remarks that ensuring treatment and protecting staff and patiens from from risk of infection must be prioritized over the concerns about possible diversion of medications of due diligence.
First, India has decided to adopt A more flexible for dispensing of medications such as buprenorphine, naloxone and methadone, which is effective against opiate disorders. Guidelines and procedures have been formulated and delivered to service providers. Consequently a large proportion of patients have continued receiving their medications uninterruptedly during the pandemic in the take home manner. While the long term impact of this change in the dispensing procedures and guidelines remains to be seen, the early experience indicates that the patients and health providers have welcomed these changes and contrary to the prevailing concerns, no report of significant divergent and adverse consequences have emerged so far. The pandemic has also brought to forefront the importance of using digital technologies to conduct the routine activities of human life. India has also taken rapid strides in telehealth and has been developing and disseminating telemedicine telepsychiatry guidelines for the health providers. However prescription of medications for preventing diversion and procurement of the same by a patient remains a challenge. We took the UNODC material that is a set of guidelines to the member states regarding safe and efficient use of telehealth mechanisms to improve access to controlled medications and secondly to collect analyze and disseminate data on the adverse influence of the pandemic on availability of controlled medications for treatment orders as well as the impact of various measures adopted by the member states to address these challenges. Thank you very much chair and ladies and gentlemen.
CHAIR: Thank you for your statement. I now give the floor to Venezuela
VENEZUELA: Bring us the floor again regarding this agenda item we included out contributions in a previous statement we had 5C and D together thank you
CHAIR: thank you that’s so very well organized you so much
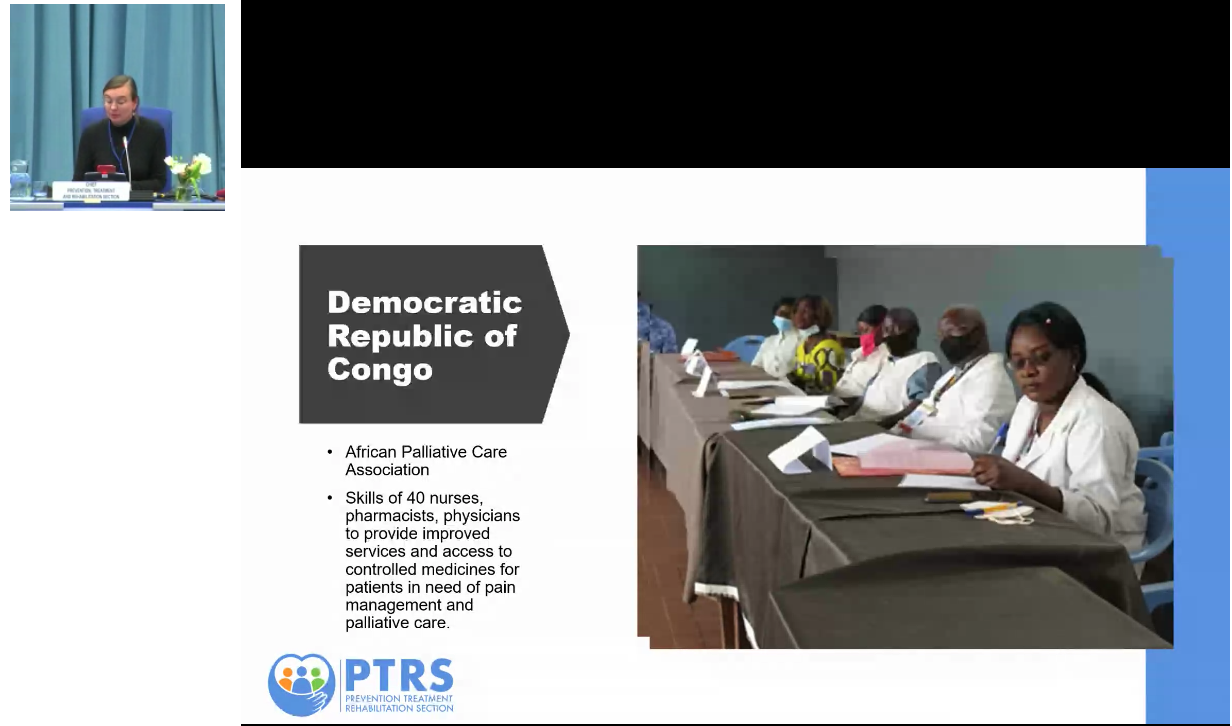
Belgium: Belgium aligns itself with the statement made by France on behalf of the EU and its member states. During the 65th session special attention will be given to the additional efforts needed to scale up the implementation of international drug policy commitments on improving availability and access to control substances for medical and scientific purposes . On a day to day basis, millions of people around the world suffer the lack of access to controlled medicines. This is getting even more critical in emergency situations. Think about the COVID 19 pandemic, but also about countries facing natural disasters or situations. Countries and humanitarian aid medicines face considerable challenges in the timely support of and access to controlled substances to these kind of emergency sites. In this regard, Belgium has served the last few days 4.6 million euros worth of medicines and medical equipment to Ukraine among which narcotics anesthesia. Belgium strongly condemns the intervention committed by Russia in Ukraine which are impacting millions of people and violating our common principle as United Nations. Throughout the year and with financial support from Belgium, UNODC will carry out a series of awareness raising events meetings and activities to call upon member states either to analyze and revise their existing policies, or to support countries in this exercise. This initiative is called “no patient left behind”. We warmly thank the participants and supporters. We are also looking forward to the one day special form on this topic that will be organized in October this year. Additionally, we also continue to support African countries in the need of technical assistance, and truth joint global program on access to control drugs. In 2020-2021 Belgium financed projects and trainings in the Democratic Republic of combo in firstly identifying gaps and opportunities to support increasing access to essential controlled medicines and secondly in building knowledge and skills necessary to support healthcare workforce to deliver safe, high quality pain management and palliative care to patients in need. Amongst many others one of the lessons learned is the importance of a local manufacturing of essential medicines such as oral morphine. Belgium as part of team Europe has invested over 14.5 million euros in equitable access and quality assured local production of health project products in Africa in support of the African Union ambitions to reduce the dependence with 60% by 2014. Our partnership in this regard focuses on first access to technologies and tech transfers, and secondly, in enabling environment such as skills and trainings but also strong regulatory environment for quality insurance. Thank you
CHAIR: Thank you very much for your statement. Should we try to connect again with the Russian Federation? You have the floor. No? We are having connection issues. Let’s go with USA then,
USA: thank you Mr. Chairman no person should suffer from untreated pain or be denied needed medicines. The drug treaties require us to ensure the availability of narcotic drugs and other controlled substances for medical and scientific purposes while preventing their diversion and international trafficking, but we are focused on the proliferation of news psychoactive substances and design substances. We are also committed to addressing barriers related to access and availability of controlled substances for medical and scientific purposes. International scheduling should not introduce barriers to access and availability, as the drug control conventions obligate state parties to ensure controlled substances are available for medical and scientific purposes. International control decisions should be a company with recommendations to implement these decisions at the national level. International control does not trigger an automatic ban at the substance for medical and scientific purposes. To help us address this gap we asked UNODC, INCB and WHO to provide information on the source of barriers to access and availability thank you
CHAIR: I now give the floor to Australia for their intervemtion. No sound? Ok, lets move on. We will continue discussing Item 5 E. on the matters arising from the international drug control treaties, and now I may ask the officer of UNODC to introduce the item
5. e) Other matters arising from the international drug control treaties
CHAIR: I now give the floor to Australia for their intervention. No sound? Ok, lets move on. We will continue discussing Item 5 E on the matters arising from the international drug control treaties, and now I may ask the officer of UNODC to introduce the item
UNODC: In recent years there’s been considerable increase in the number of narcotic drugs, psychotropic substances, precursos chemicals, included in the the schedules of thr 1961 1971 conventions and the tables from the 1988 convention. Between 2014 at 2018, 68 substances were included in the 1961 and 1971 conventions, and 7 precursor chemicals included in the 1988 convention. These increases place extra responsibilities within member states to successfully implement the international drug conventions. Amongst those most affected, are law enforcement and forensic service providers who are required to analyze and identify the scheduled susbtances. UNODC continues to adopt and develop services in order to assist the work of member states. This has included the preparation of official UNODC manuals and guidelines and recommended methods for analysis of substances. Training courses for law enforcement and forensic personnle have been developed and delivered virtually. In the United Nations, our colleagues in vienna, and also in the field have taken it. Over 3,500 record standards of substances under international control have been provided to national drug testing and toxicology offices in the last year. Substances that have been recently scheduled have been included in the UNODC international collaborative exercise program, a proficiency test that supports over 95 countries worldwide. Chair, this week, the commission will consider recommendations from WHO that took place in additional three substances under control in the 1961 and 1971 convention. The recommendations from INCB took place of three precursor chemicals in the table of the 1988 convention. UNODC will respond and begin updating its multilingual dictionaries of narcotic drugs and psychotropic substances under international control and precursors and chemicals used in their manufacture, and also undertake the steps necessary to strengthen his forensic early warnings system, and adapt the scientific conferencing services to continue to effectively support member states. Thank you chair
CHAIR: As a first speaker, we will invite Algeria for an online intervention. You have the floor.
ALGERIA: (inaudible)
CHAIR: Interpretation sadly was not possible but we will ensure that the the input of the Algerian delegation is reflected in the in the proceedings um let us continue on our list and I have for the moment I have for the United states for an online intervention you have the floor.
USA: Thank you Mr. Chairman a prime aim of the drug conventions is to protect the health and welfare of humankind. Russia’s premeditated unprovoked and unjustified attack on Ukraine has already brought catastrophic human suffering and loss of life and demonstrated Russians callous disregard for its international obligations, including this aim of the treaties. The Russian Federation publicly justified its unlawful invasion of Ukraine in part by claiming that the democratically elected government of Ukraine was “drug addicts”. The drug treaties do not allow for a state to engage in the violent invasion or hostile takeover of another sovereign state in order to address substance use in that state. Under the 1988 convention states parties are required to carry out its treaty obligations, and consistent with the principles of sovereign equality and territorial integrity of States and that of non intervention in the domestic affairs of other states. The UN General Assembly similarly condemned Russia’s aggression against Ukraine deploring these actions as violations of the UN charter and called for an immediate cease of its aggression in Ukraine. We wish to echo those sentiments here in the CND as well. Thank you chair thank you for your statement do you ever gets me
CHAIR: Dear delegates we seem to have a lot of connection problems and it is close to the end of the session. We will try to connect to argentina that will be the last intervention
ARGENTINA: In the concern of regulatory agencies is the possible adulteration of medicines under agenda item 5 regarding the treaties and changes in the scope of control of substances. It was pointed out that in the WHO’s expert committee have been examinations of psychoactive substances including MDMA and the cannabinoid receptors, in the note by the secretariat, the following data was provided on synthetic cannabinoids and it was clarified that in reality the substance has not been officially studied by the WHO. It is not currently under international control. This substance has a similar chemical structure to that of several synthetic cannabinoids that are on list two of the 1971 convention. It has an impact on the central nervous system it represents a risk to public health given that its consumption has been linked to death and merchants hospital emergency room admittance however the report points out that there is not enough information on overdose cases. There has not been studies in animals or humans that indicate that it’s inappropriate use or could lead to addiction, however, I would like to point out that the synthetic cannabinoids does not have any known therapeutic use and the data obtained so far come from drug seizures. For that reason, in accordance with the concern of the regulatory agencies, it would be of interest to continue exchanging information and furthering the analysis of data on synthetic cannabinoids in those conditions. That is when they can be used to adulterate pharmaceutical products and that way they could possibly be included in the list because they are similar to other substances. Thank you
CHAIR: Thank you. Dear delegates, it is close to 7, so I will finish the meeting for today. Thank you to the interpreters and secretariat for your support, and thank you everyone for your patience. We’ll see you again tomorrow at 10am