Organized by the United Kingdom with the support of Canada, Estonia, and the United States of America, and the UNODC Laboratory and Scientific Section.
The purpose of this side event is to discuss the experiences of member states and strategies that they have taken to tackle fentanyl and synthetic opioid markets with a view to considering how these interdiction controls could be applied to other member states
Moderator: Ambassador Corinne Kitsell – Permanent Mission of the United Kingdom
Purpose: to discuss the experiences of MS and strategies that they have taken to tackle fentanyl and synthetic opioid markets, and consider how these interdiction controls could be applied to other MS.
Panellists:
The harms of fentanyl and synthetic opioids and the global scale of the problem
Dr Justice Tettey – Chief Laboratory and Scientific Section, UNODC – The harms of fentanyl and synthetic opioids and the global scale of the problem
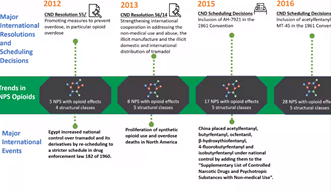
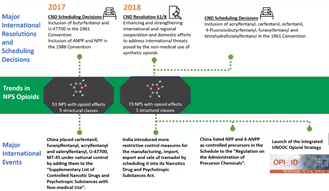
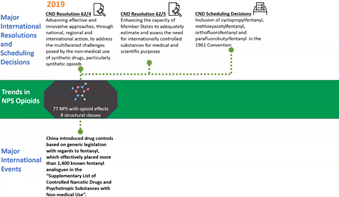
Opioids is a generic term for a range of substances. Many of these essential for management of pain – but there’s always been a worry that they will be used extra-medically. Non-medical use can have severe consequences. 1970s and 1980s – fentanyl appeared on Nth American markets. Since 2010s, crises emerged. Gradually moving to other areas, including Oceania. Rapid emergence of NPS with opioid effects. All within background of low level of access in low-income countries. Since 2015, 80 NPD with opioids effects have emerged – five-fold increase. Spectrum of interventions: number of CND resolutions and scheduling decisions since 2012. A number of countries have scheduled fentanyl analogues. We have very forward-looking measures – China in 2019 – 1400 known fentanyl analogues scheduled. Will hopefully be another one controlled tomorrow. Brorphine appearing on market. UNODC UN Toolkit on Synthetic drugs can be used.
The situation in the UK
Lawrence Gibbons – Head of Drug Threat, UK National Crime Agency – The situation in the UK
I’m an ex-police detective with 40 years experience. 2017: evidence in UK of synthetic opioids. 2020: ACMD report highlighted dangers of fentanyl and rise of new synthetic opioids. UK keen to ensure they don’t miss warning signs experienced by other countries. Strong guidelines in UK for prescribers ‘Opioids Aware resource’. Detection is vital and has started in UK. Legislation includes long standing under generic control.
Most fentanyl variants and analogues are captured by the generic control under Class A of the Misuse of Drugs Act (MDA) 1971. Those supplying, producing, importing or exporting fentanyl can face life imprisonment when sentenced. The rates of registered deaths involving fentanyl variants in the UK had increased over the past decade – the UK remains alert to the fentanyl risk, e.g. new synthetic opioids detected – isotonitazene and brorphine, likely to fall outside the generic control under the MDA 1971. Toxbase and IONA – identification of NPS in UK.
2017: Seizure of heroin containing fentanyl – then fentanyl related deaths. Response was to take action on distribution networks.
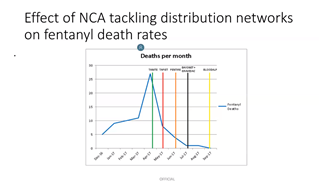
Blue line – deaths per month – vertical lines are various National Crime Agency operations, when taken out on the darknet. Rate of death peaked in 2017. Enforcement successes. “UK Bargains” seizure.
Border Force detection capabilities – through raman spectroscopy – sometimes give false readings. Fast parcel detections have occurred – usually sent to individuals. No way of targeting these shipments. Collaboration with INCB very useful, Project ION – rapid sharing of information on shipments. UK is domestically monitoring new substances.
Learning from the experiences of others
Stephen “Mac” McConachie – Chief CBP Officer, U.S. Customs and Border Protection – Learning from the experiences of the USA
Overdose and drug poisoning deaths very high in US. Six points we’ve taken:
- Tackling fear: distribution of naloxone
- Training canines: seizures doubled. Canada and Mexico also training canines. Worried about harming the dogs – but they were already being exposed.
- STOP Act: Detection on mail parcels. Would like to call out China for setting the bar high here. Importance of Advance Electronic Data. Embrace science of drug chemistry
- INTERDICT Act
- CBP’s 24-hr virtual laboratory
- CBP’s drug seizure dashboard: uploading to IONICS. We would be remiss to not share our processes with others working in similar fields.
Douglas Culver – Policy Advisor, Public Safety Canada – Learning from the experiences of Canada
Previous RCMP officer. Canada’s fentanyl problems started in 2007. Started to hear that there were clan labs in the US, and diversion of medical fentanyl. Border force was first key line of defence. CBSA were interdicting small amount through postal services – we all know how harmful fentanyl can be in small amounts. Were limited by legislation. As border interdiction improved, we started see Canadian based clan labs open.
Prior to 2016 – no precursors for fentanyl based products listed in our acts. Working with Health Canada to find precursors – production still going on. Organised crime and synthetic opioids – organised crime groups already involved in synthetic drugs adapted quickly. Domestic precursors dried up, so smuggling of precursors from Asian sources became the norm. Hundreds of kilogram quantities began showing up in country. “Super” labs now produce synthetic opioids.
Domestic precursors dried up, smuggling of precursors from Asian producers. Large pill presses, tabletting operations, mostly in Western Canada. Starting to distribute to foreign markets.
Designated devices: the two western provinces of Canada adopted legislation. Federal legislation also came into effect in 2018 in response to the importation of pill presses. There is a high demand on the street for OP 80’s, M 30’s. Pill presses were in large demand for mass production facilities.
Lessons learned: large increases in drug overdoses – not going away. Organised crime adapted to emerging markets. There must be concerted changes in our approach. Trying to close as many doors as possible. Legislation needs to evolve faster than the illicit market.
Next steps: Designated Devices Research Project – trying to control the pill presses coming into the country. Offering Drug Stigma Awareness Training to improved interactions between law enforcement and PWUD. Continuing to work with Health Canada, and international partners.
Ain Peil – Drug Policy Advisor, Estonia Ministry of the Interior – Learning from the experiences of Estonia
Mostly speak to our long experiences with fentanyls. Our opioid problems started in 1990s – beginning of 00’s fentanyl took over the market. Resulted in a number of overdose related deaths. Fentanyl mostly injected or smoked – about 15 different forms on the market at the time. Major takedowns in 2017 – resulted in disruption of fentanyl markets. OD deaths dropped immediately – fentanyl production also dropped significantly. Only one home lab dismantled in 2019. Wider perspective: Estonian drug situation: fent users started looking other ways – over borders, to darknet, also turning to other drugs. Increase in treatment and harm reduction services. Current state of play: keep OD deaths low, but future is very uncertain
Focus from supply to demand reduction over the last 10 years. Need more cross border review and analyses. Lessons learned: Estonian success story – hard to duplicate – our country is very small. Focus on other drugs must remain too, not just on fentanyls. New services must be considered: experiences – drug testing, drug consumption rooms, cannabis regulation should be considered. If situations like this emerge, we need to be well informed. Market controls – we need to adapt. More than happy to get in contact.
For any questions relating to this side event please contact Kerry.Eglinton@homeoffice.gov.uk
