Item 5. Implementation of the international drug control treaties (continued)
(a) Changes in the scope of control of substances
Chair: We are waiting for the delegation from WHO to present the substances. I have the pleasure to invite Mr, to present substances: N-pyrrolidino isotonitazene and N-desethyl etonitazene to be placed in.Schedule I from the single convention on narcotic drugs 1961 as amended by the 1972 protocol.
WHO: N-pyrrolidino isotonitazene is a synthetic opioid that acts as a full agonist of the opioid receptors. In animals it has similar potency to morphine and fentanyl. Its presence has been reported in many countries and regions although the extent of use is unknown. It has been analytically confirmed in fatal and non-fatal cases of overdose, including in cases in which it was the only substance detected. In conclusion N-pyrrolidino isotonitazene is a syntethic opioid liable to abuse to abuse and produces effects similar to those of others that are controlled in Schedule I. It causes substantial harm and has no known therapeutic use. Therefore WHO recommends it to be added to Schedule I.
Chair: I invite the commission to take a vote. Let me remind that a simple majority of people present is required. I now call the vote
Argentina, Armenia, Australia, Austria, Belgium, Burkina Faso, Burundi, Chile, China, Colombia, Dominican Republic, Finland, France, Germany, Ghana, Guatemala, Honduras, Hungary, India, Indonesia, Italy, Japan, Kazakhstan, Kenya, Kyrgyzstan, Lithuania, Malta, Mexico, Morocco, Kingdom of the Netherlands, Nigeria, Pakistan, Peru, Poland, Portugal, Singapore, Slovenia, South Africa, Spain, Switzerland, Thailand, United Arab Emirates, United Kingdom, Tanzania, United States, Uruguay, Zimbabwe
Mexico: A motion of order, there was a country that was not mentioned.
Chair: After Colombia we have Cote d’Ivory. Now I call the members on the commission not in support of the recommendation by raising their country signs. None. Now I call the ones who abstain to indicate their abstention by raising their country signs.
Secretary: Qatar.
Chair: 48 in favor, none against and 1 abstention. The commission has agreed on including N-pyrrolidino isotonitazene in the convention. Now I call WHO to present the next substance N-desethyl etonitazene.
WHO: N-Desethyl etonitazene is a synthetic opioid and a metabolite of etonitazene which is controlled under Schedule I. Studies of receptor binding in vitro indicate that N-Desethyl etonitazene is a full agonist with greater potency than morphine and no control studies on the dependency potential in animals or humans have been reported. However, it would be expected to produce dependency similar to other opioids such as morphine and fentanyl. It has been reported in at least 10 countries with unknown extent of use. It has been confirmed in at least three deaths including when no other opioids were involved and in non-fatal overdoses. It could theoretically be converted into a control substance, although it has not been demonstrated. Its use causes substantial harm, including death. It has no known therapeutic use. The WHO recommends that it is added to Schedule I.
Chair: I invite the commission to make a vote in N-Desethyl etonitazene in the Schedule 1 of the 1961 convention. I now call the members of the commission in favor of including the substance in Schedule 1 of the convention to raise their country signs.
Argentina, Armenia, Australia, Austria, Belgium, Bolivia, Burkina Faso, Chile, China, Colombia, Dominican Republic, Finland, France, Germany, Ghana, Guatemala, Honduras, Hungary, India, Indonesia, Italy, Japan, Kazakhstan, Kyrgyzstan, Lithuania, Malta, Mexico, Morocco, Netherlands, Nigeria, Pakistan, Peru, Poland, Portugal, Qatar, Singapore, Slovenia, South Africa, Spain, Switzerland, Thailand, Ukraine, United Arab Emirates United Kingdom, United States of America, Tanzania, Uruguay, Zimbabwe
Chair: Now I call the members of the commission not in favor. None. Now I call the members of the commission that abstain. None. Thank you. Total of 49 votes in favor, 0 against and 0 abstain. Then I declare the commission has decided to include N-Desethyl etonitazene in Schedule I.
Now we move to Schedule II.
WHO: MDMB-FUBINACA is a synthetic cannabinoid that binds to CB1 and CB2 receptors with high affinity and is a potent full agonist at both receptors. Its effects are similar to those of other potent CB1 agonists that are currently controlled under Schedule II of the Convention on Psychotropic Substances of 1971. No controlled studies of the effects of MDMB-FUBINACA have been reported. In animals, it has been shown to produce behavioural effects consistent with delta-9-THC, with the effects lasting many hours. In humans, it produces symptoms typical of high doses of cannabinoids, including agitation or sedation, vomiting, short-term memory loss, salivation, rhinorrhoea, mydriasis, tachycardia and anxiety. No studies of the dependence potential of MDMB-FUBINACA in animals or humans have been reported. Its effects at CB1 receptors suggest that it would produce dependence similar to that produced by delta-9-THC and other synthetic cannabinoid receptor agonists. Countries in two regions reported presentations for treatment of drug dependence due to the use of MDMB-FUBINACA. MDMB-FUBINACA is a synthetic cannabinoid receptor agonist administered by smoking plant material sprayed with the substance or inhaling vapour after heating. Its mode of action suggests the potential for dependence and the likelihood of abuse. Its use has been associated with a range of severe adverse effects, including death. These effects are similar to those produced by other synthetic cannabinoids that are placed in Schedule II of the Convention on Psychotropic Substances of 1971. MDMBFUBINACA has no therapeutic use and we recommend it to be added to Schedule II.
Chair: I invite the commission to make a vote on the scheduling of MDMB-FUBINACA to be included in Schedule II of the 1971 Convention. I call only the countries in favor to raise their country sign
Argentina, Armenia, Australia, Austria, Belgium, Bolivia, Burkina Faso, Chile, China, Colombia, Dominican Republic, Finland, France, Germany, Ghana, Guatemala, Honduras, Hungary, India, Indonesia, Italy, Japan, Kazakhstan, Kyrgyzstan, Lithuania, Malta, Mexico, Morocco, Netherlands, Nigeria, Pakistan, Peru, Poland, Portugal, Qatar, Singapore, Slovenia, South Africa, Spain, Switzerland, Thailand, Ukraine, United Arab Emirates United Kingdom, United States of America, Tanzania, Uruguay, Zimbabwe.
Chair: Now I call the countries not in favor of the recommendation: None. Thank you. Now I call the countries abstaining. None. Thank you. Total of 49 in favor, 0 against and 0 abstain. Therefore I declare the commission has decided to include MDMB-FUBINACA in Schedule II of the 1971 convention. I give the floor to China.
China: China would like to congratulate the scheduling of the 3 substances. China has already scheduled many of these substances. I think this will have a very positive impact because I find this very necessary. Thank you very much.
Ghana: I would like to recommend changes. Falling on the convention, addition and retentions of substances under international scheduling. 1) The proposed inclusion of N-pyrrolidino isotonitazene reflected on the potential for global harm. 2) The retention of coca leaf to continue the long consensus of a substance within strict regulations globally. 3) From a national perspective the commission that the substance tramadol has not been scheduled. Ghana remains committed to information sharing to ensure that national control falls in line with international obligations.
Kenya: My delegation notes that decisions have far reaching consequences, ensuring balance between availability for medical purposes and law enforcement. (…) Such assistance should include regulatory frameworks, supply and demand control, bolstering national capabilities, and improving access for medical purposes. We welcome closer collaboration between CND, WHO, INCB, UNODC and regional organisations. Transparency and inclusivity of the scheduling process are vital. Meaningful involvement of communities and civil society is vital to integrity. We request that the WHO consider evaluation of tramadol and discussion of consideration of ketamine. Our region has further witnessed use of veterinary medicine such as xylazine and drug mixtures. We call for further advice on control measures. All relevant states and stakeholders to safeguard HR and strengthen rule of law.
USA: We view scheduling as means for us to protect citizens as we tinker with chemicals to bypass regulations, this is how we say “not so fast”. Scheduling is not only a decision and if experience is a guide there are harder choices to come. I recall Max Colby who on August 14th 1941 was killed in Auschwitz, because of his death by drugs he is venerated as patron saint of drug addicts. Colby was only killed when he volunteered to take the place of another prisoner. We are not called to make that sacrifice but we hope for multi-lateral efforts to thwart evil. How many actual addicts see us today as their champion? How many traffickers see us as their scourge? The world here is nothing like the criminal world out there, where cocaine and speed are bought and sold. We diplomats are removed from this world, one reason is we have outsourced our decision making. When we ask how ambassadors will stop trafficking, they deflect. They say we have given money to the UN office on capacity building. When pressed for details, they are tonguetied or indifferent. Questioning efficacy has become the third rail of counter narcotics assistance. We have aspirational failure, modesty of our aims. When you read statements at last year’s CND this is clear – one important country said the key to stemming drug flows is cooperation without confrontation, whatever that means, another referenced the importance of yoga to protect youth. Another country blew the opportunity to counter charges against them by putting the CND audience to sleep by talking about openness, inclusiveness, and shared benefits. We have no time for empty talk. When we target traffickers or captured cartel leader Nicolas Maduro, declare fentanyl and weapon of mass destruction. When we convened the Shield of the Americas last week to unleash an offensive against narcoterrorism. We focus on supply reduction, but we have not forgotten demand. In closing, let’s think of Colby this week, lives even here in Vienna lie in the balance. Ask all those who debate resolutions to ensure we have concrete actions documented at CND next year. We can’t be patron saints but shouldn’t settle for less than being patron diplomats
Nigeria: We have become a major destination and transit point for shipments and non-medical use of opioids, including those banned and tightly regulated. This poses significant risk and widespread drug dependence, increased in criminality and aggravated a fragile security situation. Unlike other opioids, tramadol is not under control. As a result it is inexpensive and accessible. Traffickers have abused this and flooded the market in our region with high dose variations. Tramadol is a major public health concern in our region. It is linked to criminal networks and the financing of terrorism. This underlines the need to strengthen drug control measures. With support of UNODC we have taken significant steps to disrupt the supply chain of substances. Enforcement alone cannot fully address challenges. In absence of scheduling the use will expand with further problems for public health and safety. We call for appropriate scheduling of tramadol by CND based on assessment by WHO. This would strengthen regulation and restrict diversion. This measure will contribute to protecting vulnerable populations and public health.
IFRCRC: 10 years after UNGASS we have an important opportunity to reflect on progress and ensure policies are responsive to reality and evidence based. Over the past decade, we have contributed to this aim through the Rome Consensus initiative. What began as platform to reflect on UNGASS has grown to a broader alliance bringing together health professionals, law enforcement, academics, and civil society. We promote holistic and balanced framework connecting prevention, treatment, harm reduction, and reintegration which too often work in isolation. Translate global commitment into concrete action at community level. Constructive dialogue between health and justice, and civil society and public authorities. Progress is unfortunately limited by absence of a universally agreed definition of harm reduction within the UN system. Harm reduction should not be treated as a partisan banner, much of this polarisation is caused by absence of shared language by clearly defined meaning and applications. Recent reports show funding cuts are already forcing harm reduction and treatment programs to scale back or close services. Losing these programs will not only cost lives, but risk reversing decades of progress in preventing HIV, Hepatitis C, overdose deaths, and punishing people with drug use disorders. Ensuring access to treatment is in the interest of every community and thus every member state. We must recognise the simple reality – recovery can’t be imposed. Drug policy will ultimately be judged not by substances we control, but by lives we protect. The Red Cross and Red Crescent Societies stand ready to continue working alongside governments, communities, and partners to turn shared commitment into solutions that leave nobody behind.
ENCOD: I am speaking on behalf of Dejusticia, Elementa DDHH, ENCOD and the Coca Alliance for Peace, civil society organisations working to uphold human rights and reform drug policies in Latin America. As organisations participating in the critical review process of the coca leaf, we wish to express our deep concern at the decision of the WHO and its Committee of Experts on Drug Dependence to keep this plant on Schedule I of the Single Convention on Narcotic Drugs. Firstly, we would like to state that the critical review report missed an opportunity to promote measures to protect the traditional uses of coca and enable legal uses for medical, scientific and industrial purposes for peasant, mestizo and Afro-descendant populations. We believe that the lack of inclusion of the social sciences in the Expert Committee, as well as its limited concept of science, led to the dismissal of the so-called ‘grey literature’ in which most of the information systematised by the indigenous and mestizo communities that have an ancestral relationship with the coca leaf is found. Thus, the report has an obvious bias in the selection of studies and in its conclusions. Discarding grey literature and information generated by rural communities and the social sciences disregards the concept of science as defined by UNESCO and by General Comment No. 25 of the CESCR. By acknowledging that there is no scientific evidence on aspects such as nutritional values or safety, the WHO falls into the trap of the international narcotics regime: there is no evidence to declassify coca, but such evidence cannot be constructed because it is subject to strict controls. In Colombia, obtaining permits to research the coca leaf requires years of paperwork and advocacy. In this way, the WHO and the Committee of Experts reinforce the obstacles and biases imposed by the international control regime on the study of the coca leaf and ignore the WHO guidelines for research and examination of traditional medicine, which includes plants such as the coca leaf. Secondly, the focus on the ‘easy’ convertibility of the coca leaf is misguided because it is not true that it is chemically ‘easy’ to extract the alkaloid from the plant, nor is it profitable for criminal organisations. Declassifying or moving the coca leaf from Schedule I will not affect the measures implemented by States to combat the illegal production of cocaine. Cocaine production is a complex transformation process that requires knowledge and expertise. Although rural communities in Colombia have learned to extract coca base paste, cocaine production is carried out by criminal groups capable of developing the necessary logistics. The UNODC itself recognises that the synthesis of the alkaloid requires multiple procedures and the use of chemical inputs that are increasingly restricted. It is not true that anyone can extract cocaine from products derived from the coca leaf. In a country like Colombia, where illicit crops provide raw materials for the cocaine industry, it would be unprofitable to use traditional products or alternative uses to extract the alkaloid. Although cocaine is extracted from the leaf, extracting even 1 gram of cocaine from the coca leaf is a voluminous and costly process. It is estimated that to produce 1.5 kilograms of coca base paste, more than 750 kg of fresh coca leaf must be used, an amount that is almost impossible to achieve through herbal teas. The approach taken by the Expert Committee on convertibility even contravenes the provisions of the “guidelines on the WHO review of psychoactive substances for international control”, which state that a substance is considered convertible if it is of such a nature that, due to the ease of the process, “it is feasible and profitable for a clandestine manufacturer to transform the substance in question into controlled drugs”. The critical review process was an opportunity to correct the historic mistake made by the international community in including this sacred plant in the international control regime. Thus, the control system has proven incapable of adapting to the changes required by the rights of indigenous peoples, diverse knowledge, and the possibility of making use of the scientific benefits of a stigmatised plant.
(e) Other matters arising from the international drug control treaties
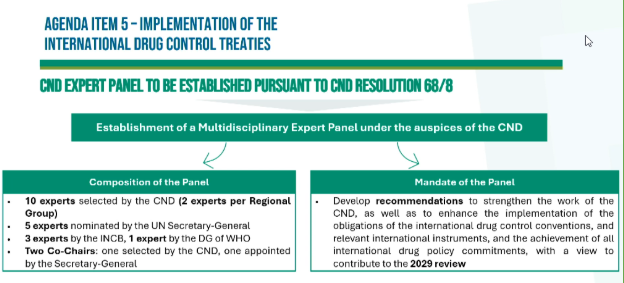
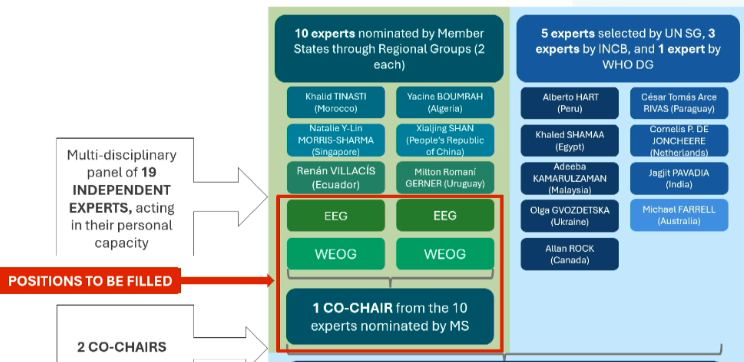
Chair: Thank you, now moving to agenda point 5e, the expert panel. The Commission decided to establish a disciplinary panelof 19 experts: 10 members selected by commission + 2 nominations from five regional groups+ 5 five members selected by the Secretary General + 3 selected by the INCB + 1 by the director of WHO acting in their personal capacity to prepare a clear, specific set of recommendations, aimed at implementation of international drug control treaties. During its reconvened 68 session, the Commission endorsed the nomination submitted by regional groups for membership in the expert panel established pursuant to commission resolution 68 slash six. The experts were endorsed for certain groups but the Commission further noted that the scene to the Eastern European group and the Western European and other states group had not yet been filled. It was noted that these remaining seats would need to be filled no later than at its regular session in March 2026 and that consensus within regional group not be reached, the commission would be required to proceed to election to fill the outstanding basis. The commission would also need to appoint the co chair at the regular 69th session as set up resolution 68/6.
(Experts selected by CND: Ukraine, Malaysia, Canada Egypt, Peru; INCB: Paraguay, Netherlands, India; WHO: Austrlia; SG: Canada)
Secretariat: introducing the process (pictured below) and remains fully committed to supporting the work of the Commission.
Chair: We shall now proceed to the selection of experts on to the panel. Delegations wishing to make statements can do so once the appointment of 2nd cochair has been completed on Thursday morning.
These rules apply to subsidiary bodies established by ECOSOC, such as the CND:
Rule 66 — Elections: All elections in a functional commission are to be conducted by secret ballot. However, if there is no objection from the members present, the commission may decide to proceed without a formal ballot for an agreed candidate or slate.
Rule 67 — Method of Election: When there are multiple elective places to be filled at the same time under the same conditions, those candidates who: obtain a majority of the votes cast, and receive the largest number of votes, up to the number of available places, shall be elected. If after the first ballot fewer candidates reach the required majority than there are places to be filled, the commission shall hold additional ballots to fill the remaining vacancies.
Rule 70 (Procedure when two or more elective places are to be filled): When two or more elective places are to be filled at one time under the same conditions, those candidates, in a number not exceeding the number of such places, obtaining in the first ballot the majority required and the largest number of votes shall be elected. If the number of candidates obtaining such majority is less than the number of places to be filled, additional ballots shall be held to fill the remaining places, provided that if only one place remains to be filled the procedures in rule 69 shall be applied. The ballot shall be restricted to the unsuccessful candidates having obtained the largest number of votes in the previous ballot, but not exceeding twice the number of places remaining to be filled. However, in the case of a tie between a greater number of unsuccessful candidates, a special ballot shall be held for the purpose of reducing the number of candidates to the required number; if a tie again results among more than the required number of candidates, the President shall reduce their number to that required by drawing lots. If such a restricted ballot (not counting a special ballot held under the conditions specified in the last sentence of paragraph 2) is inconclusive, the President shall decide among the remaining candidates by drawing lots.
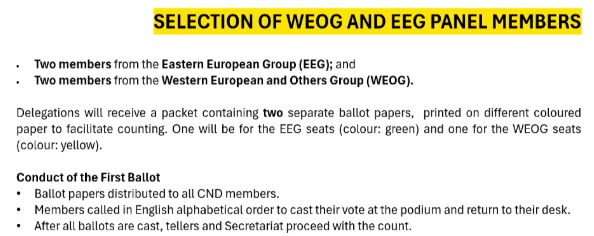
Secretariat: Clarification on majority and selection of panel members from EEG and WEOG (see slide)
 As per the Rules of Procedure – Rule 61, once the voting is underway, no representative may interrupt.
As per the Rules of Procedure – Rule 61, once the voting is underway, no representative may interrupt.
Chair: Representatives of Egypt and Chile have agreed to serve as tellers. As the tellers are doing their work we will continue in order to save time. I will announce the names of experts from EEG and WEOG. I would like to remind members that no representative may interrupt with voting except on point of order in connection with the actual process of voting. The ballot will now begin. I will ask ballot papers to be distributed to the members of the commission present in the room. I ask to confirm that the ballot box is empty. The secretary will call members in alphabetical order to come to the podium.
Secretary: I will give delegates 2 minutes because the ballots were just distributed. Kindly make sure papers are also folded. Can everybody remain seated, please?
Chair: Now everyone already has the ballots and votes have been cast. I ask everyone to remain seated and quiet, please.
Secretary: Argentina, Armenia, Australia, Austria, Belgium, Bolivia, Burkina Faso, Burundi, Chile, China, Colombia, Cote D’Ivoire, Dominican Republic, Finland, France, Germany, Ghana, Guatemala, Honduras, Hungary, India, Indonesia, Italy, Japan, Kazakhstan, Kenya, Kyrgyzstan, Lithuania, Malta, Mauritania – not in the room I think so we move on to Mexico, Morocco, Kingdom of the Netherlands, Nigeria, Pakistan, Peru, Poland, Portugal, Qatar, Singapore, Slovenia, South Africa, Spain, Switzerland, Thailand, Trinidad and Tobago – I think not in the room so we move on to Ukraine, United Arab Emirates, United Kingdom, United Republic of Tanzania, United States of America, Uruguay, and the last member, Zimbabwe please.
Chair: The ballot process is now complete, I declare the voting closed and I ask the tellers to count the votes. I suggest we proceed with remaining speakers until tellers complete the counting. I invite Slovenia
Item 3. General Debate
Slovenia: In addition to the statement of EU, allow me to share several remarks. We value the role of the UNODC who provides a platform for exchanging experiences and shaping common responses to the production, trafficking and use of illicit drugs at the global, regional and national levels. Slovenia decided to increase financial support to UNODC, particularly in early prevention. We are not immune to the challenges of drug abuse. We observe the emergence of new psychoactive substances, and our response is comprehensive and balanced. Only coordinated and sustained action can lead to lasting results. Our Ministry of Health promotes evidence-based measures and focuses on prevention, early intervention, harm reduction, and social integration. Special attention is given to vulnerable groups such as young people. We consider addiction as an illness, as people need medical care, social assistance, and rehab, not stigma. We finance programs that support their reintegration into society. Reducing supply remains one of the guiding principles of a comprehensive drug policy. Organized crime groups are adaptive and we observe that synthetic drugs are easily accessible in shops and online, including vapes and edibles, and they lead to health risks. We support global action in regulation because individual efforts are not enough for such a problem. Slovenia gives importance to regional cooperation, and we intend to strengthen cooperation with countries of Western Balkans, UNODC and Pompidou Group of the CoE.
Poland: Poland fully supports the EU statement and focuses on protecting human life and dignity. We reject the death penalty in all situations, including extrajudicial killings. We oppose war and condemn Russian military aggression against the independent state of Ukraine. We emphasize the growing problem of synthetic opioids which pose a challenge to public health and law enforcement. One of last year’s resolutions tabled by Poland on behalf of the EU addresses this. The EU is increasingly threatened by these substances. We recognize the link between mental health and drug use and stress the importance of self-care and psychological well-being of children, adolescents, and women. 10 years after UNGASS, the outcome document remains relevant and while progress was made there are still significant challenges and need for cooperation and shared responsibility. In public health we highlight preventive and treatment measures that place drug and drug dependence in a wider framework of addiction including alcohol related problems and behavioral addictions. We stress the importance of evidence-based prevention and member states have shown commitment to evidence-based policy by implementing quality standards . Building coalition is crucial as cities and communities play a significant role in universal, selective, indicated, and environmental prevention measures. The effort would be incomplete without the vital contribution of civil society which plays a key role in addressing drug-related challenges and supporting people affected by addiction, and must have reliable access to public and international funds.
Bulgaria: We align with the statement from the EU and recognize that the world drug situation remains a complex and multifaceted challenge requiring a balanced approach and evidence-based human rights-centered approach, as well as shared responsibility and full respect for international law. Our national strategy reflects those principles and aims to reduce negative consequences of the spread and use of narcotic drugs and analogues, focused on improving health security and quality of life for society. Drugs remain a serious challenge with long-term consequences for the future of young people and for the social environment, economic stability and rule of law. We will address this with engagement with the local prevention network. We are observing a positive trend in improving results related to the detection and investigation of crimes. This concerns offences of national nature and international criminal activities. Bulgaria addition to Schengen has further strengthened our commitment to border management with cooperation within the EU and partner countries and international law enforcement authorities. In 2025 around 7000 drug operations were carried out, we have 13% increase in registered drug related crimes, 24% decrease in solved crimes. Police dismantled more than 40 small to medium-size synthetic drug laboratories and many illegal cannabis farms. The cooperation between UNODC and the National Institute Forensic Science of Bulgaria will lead to more informed and effective responses to drug-related threats and new psychoactive substances which are highly varied and evolve rapidly, requiring constant monitoring and coordination. Only true, consistent, and coordinated efforts can limit the spread of narcotic substances and ensure a safer and healthy future for younger generations and the whole community.
Indonesia: associates with G77 statement and adds that our national capacity is concerned with growing opacity and danger of global drug situation, proliferation of synthetic drugs, exploitation of maritime roots and use of digital platforms for illicit activities. This all underscores the need for not only technical solutions but collective leadership. Indonesia guarantees rehabilitation for those affected by drugs and commits to reinforce intelligence and national coordination. (…) Arrest of 1174 suspects, seizure of more than 4 tons of methamphetamine and 2.1 tons of cannabis, elimination of 127800 square meters of cannabis plantation, destruction of 224.5000 plants, confiscation of 144 billion (…) Six narcotics related money laundering cases. The quality of rehabilitation services complies with national standards and was adopted by 4400 institutions with community involvement. Innovations facilitate a more accessible and dignified process. We focus on prevention through integration of anti drug education in schools, strengthening families and development of drug free initiatives. These features critical investment in national resilience and future generations . At CND Indonesia highlights 3 fundamental priorities 1) uphold global drug control systems, opposing weakening of international conventions and normalization of drug use. 2) global cooperation against crime with emphasis on maritime interdiction and intelligence 3) committed to promote human evidence by ensuring recovery systems are accessible and uphold the dignity of those affected by drug advances. Indonesia supports initiatives to advance the ministerial declaration and control conventions and is committed to fostering international cooperation against transnational crime. We are ready to work with all member states to ensure global drug policy remains effective and centered in human dignity, to build a safer and more resilient future for all. We are organizing a side event today at room M5, and have an exhibition that opens at 2pm in the margins of this session. Thank you.
Chair: I would like to recall that speaking time is 2 minutes and ask you to please stick to the time. Second, it is very noisy in the room and it is very difficult to follow the statements, so out of courtesy please remain quiet during the session. El Salvador, you have the floor.
El Salvador: CND is an essential space to coordinate international efforts, preserve public health and guarantee access to medicines. We believe in a balance between control and access that should materialize in effective public policy. In El Salvador our regulation has undergone profound evolution. We emphasize on substances classified as controlled given their therapeutic relevance and potential for misuse. We adopted a comprehensive approach bringing our legal framework in line with international commitment and strengthening oversight mechanisms regarding importing, manufacturing, storage, distribution, prescription and dispensing. This system improves traceability, reduces vulnerabilities and raises compliance standards. However, effective regulation nowadays requires innovation and our governments have driven unprecedented digital transformation in a monitoring system for controlled medicines. We implemented modern technological platforms that allow greater agility and transparency . We developed a national electronic prescription platform from controlled medicines preventing false prescriptions and allowing real time verification of availability of medicines, so that patients can identify where to find medicines they need. In production, we have 13 manufacturing laboratories which comply with best manufacturing practice, 10 of those produce controlled medicines.This positions El Salvador as the number one exporter of controlled medicines in the Central American region. We believe that international cooperation and exchange of best practices is essential for a resilient regulatory system and coordination. Our government provide technical cooperation to Central American countries and other nations. We are undergoing a process for comprehensive systematization of all procedures to reduce response times and improve transparency and resources. We work very closely and hard to achieve accreditation as a WHO listed authority. El Salvador demonstrates it is possible to build a system where access to controlled medicines or substances for medical and scientific purposes can co-exist with strict and effective controls against diversion of misuse. We will continue to collaborate in the work of CND as the highest UN body creating drug policy. We reiterate commitment and willingness to provide support so that this session can achieve results and continues to be a meeting point aimed at building innovative, supportive and sustainable solutions.
Agenda Item 5e. Other matters arising from the international drug control treaties — including votes on the Independent Expert Panel
Chair: We can now read the results of the elections of the Expert Panel. I will start with the Eastern European Group. Ballots cast 51, invalid ballots 0, valid ballots 51, abstentions 0, members present and voting 51, majority required 26. Results are as follows:
Pavel Bém, Czechia: 41 in favour
Oksana Guseva, Russian Federation: 20
Elīna Šteinerte, Latvia: 31
Pavel Bém of Czechia and Elīna Šteinerte of Latvia have reached majority. They are elected to the Expert Panel.
Results for election in the Western European and Others Group.
Ballots cast 51, invalid ballots 0, valid ballots 51, abstentions 0, members present and voting 51, majority required 26. Results are as follows:
Alexis Goosdeel, Belgium: 40
João Goulão, Portugal: 23
Virginia Patton Prugh, USA: 29
Alexis Goosdeel of Belgium, and Virginia Patton Prugh of USA, are elected to the Expert Panel.
The following experts have expressed interest in being co-chair: Natalie Sharma, Singapore, Virginia Patton Prugh, USA, and Khalid Tinasti, Morocco. As mentioned before, if there are any delegations that wish to make a general statement, they can do so on Thursday after the appointment of co-chair.
Agenda Item 3. General Debate (cont.)
Kuwait: This meeting is being held during growing challenges in the field of the anti drug fight and regarding the adverse effects that drugs have on societies and individuals. We are committed to UN principles and related treaties and conventions and efforts in terms of combating psychotropic substances. We are looking into threats of synthetic drugs to social peace and we adopt an integrated approach between a mix of strict regulation and control measures in parallel to rehabilitation services and developing prevention. We rely on international assistance and cross border efforts. Reinforcing our system, we have developed in accordance with international commitments a decree last year, no. 159, a law on psychotropic substances and drugs that responds to growing dependence on drugs in society, reclassifying offences and differentiating between drug use and related offences. We reinforced regulation of substances to protect societies. Given due attention to health, we opened a centre for drug addiction and rehabilitation in accordance to highest social and health levels and reintegrate addicts into society. We believe in non intervention in state affairs according to the UN charter. It is important to respect countries’ diversity, cultural, and religious norms when discussing drug controls. We can achieve joint objectives while respecting the specificity of states. We require international cooperation and regional cooperation and we thank the UN for efforts to implement strategy to reduce supply and demand and reinforce prevention measures. Cooperation with friendly countries to share best practices and expertise to achieve their own and common goals. Reiterate commitment to support cooperation efforts to fight drugs in all forms and enforce cooperation to achieve peace, security, and SD for all nations.
Côte d’Ivoire: The world drug problem is a complex and evolving challenge and affects the health, security, and economic reality of societies. We reiterate our commitment to the main international drug control conventions. Carried out reforms to build mechanisms against trafficking. I note we are tackling the proliferation of NPS and using more digital technologies. Regarding law enforcement, our security and defence forces are dismantling trafficking by cross border information. Social reintegration, rehabilitation, treatment and prevention remain at the heart of our strategy. Awareness raising programs have been scaled up to protect youth, involving families and community leaders. Improved access to care services for people with drug use disorders to protect dignity and act without discrimination. Rising security challenges mean we must strengthen extradition and mutual assistance for criminal matters with regional partners. It is important for transit, destination, and origin countries working in unison. We promote alternative development to promote sustainable livelihoods to communities. Investing in education, employment, women and young people empowerment. Call for strengthened technical assistance and transfer of expertise to developing countries and to countries in need. We support an approach based on compelling data that respects sovereignty and human rights. We can work together towards common objectives for health wellbeing, state security and sustainable development.
Cyprus: I have the honour to address the commission on behalf of 56 signatories. We address the CND to recall the importance of international guidelines on human rights and drug policy. Strongly reaffirm our opposition to the death penalty in all cases, in all circumstances. We recognize serious challenges related to drug control but express our concern over trends towards punitive approaches. Growing acknowledgement among members states that drug policy needs to be human rights based. Dramatic increase in application of drug policies. In the past years more than 40% of all executions were linked to drug offences. International human rights law restricts the use of capital punishment to the most serious crimes, understood as crimes of extreme gravity and intentional killing. Drug trafficking does not meet this threshold and its implementation is ineffective. This has not reduced use or ended drug trae. There is no conducive evidence that the death penalty prevents or curbs drug trafficking more than other types of punishment. Reflected in international guidelines. Capital punishment for drug offences against human rights commitments. Use of the death penalty is discriminatory and has a disproportionate impact on minorities, foreign nationals, LGBTQI+ persons. It has no place in the 21st century and time we move to a human rights based approach focusing on drug demand and supply. We agree on evidence based, integrated, multidisciplinary and balanced approach with gender responsive approach and peoples dignity at the center. 2016 UNGASS outcome promotes the well-being of society as a whole through effective scientific evidence based strategies through the needs of families, communities, comprehensive and balanced policies on a non discriminatory basis. Implement measures that tackle root causes of entering the drug trade including socio economic factors that lead to people engaging in illicit drug markets. Taking a human rights based approach to drug policy requires focusing on risk and harm reduction including meaningful involvement of communities and civil society, young people, civil society, academia, and other experts. We call on all member states to bring in a moratorium on executions, commute death sentences and ban death sentences for drug offences.
Belarus: UN drug control conventions are the foundation of the drug control system. We call on states to ensure their full and effective implementation. Our country has noted a sustained trend to reduce the number of trafficking crimes. Decrease in number of poisonings, including fatalities. Decrease in adolescents detained for drug dealing. However, the threat persists as evidenced by seizures. Our law enforcement agencies together seized more than 3 tonnes of illicit substances, the bulk of which were cathinone group synthetics. Conflict in our region has increased the number of transit efforts from EU countries towards the Russian Federation. In criminal cases we established as fact that in territories of Eastern and Central Europe there is one criminal group organising using telegram and electronic payments outside banking systems. We oppose weakening of the drug control system, including through legalisation of cannabis. This increases the likelihood of use of hard drugs. Oppose use of medical substances for non-medical purposes. Open to exchange of information on all categories of criminals including traffickers and open to joint investigations. We call on countries exerting pressure through sanctions to operate through the law and in compliance with their obligations. We stand ready to share the experience we gained and call on other countries to do likewise. We make good on obligations to provide foreign colleagues information and we expect mutually beneficial exchanges.
Morocco: This meeting is happening at an important moment for reflection, where illegal markets are going through a rapid and profound transformation. These changes throw light on response mechanisms and call on adaptation and reflection. More necessary than ever to renew and consolidate consensus and a balanced approach based on data that respects human rights and overcome challenges posed. Morocco is attached to implementation related to drug control. Strategy focused on reducing demand and therefore we have a national plan to strengthen prevention and improve access to care, promoting social rehabilitation. Our approach has a network of specialized services across the country. Supply reduction continues and drug seizures the past year amount to over 540 tonnes of cannabis resin, over 98 tonnes cannabis herb, over 1924 kg of cocaine, and over 6kg of heroin, along with 1,785,000 psychotropic pills primarily from the eastern border of Morocco. Within the framework of implementing a decision about reclassification of cannabis to allow use for medical purposes we adopted law relating to legal use of cannabis covering all activities linked to growing, transport, and use for scientific and medical use. We remain convinced the world drug problem is common and shared responsibility that demands common response based on mutual trust with cooperation. Without cooperation and mutual trust we can’t effectively combat trafficking. In respect to the Ministerial Conference upcoming in 2029 we propose collective reflection around 3 axes. 1) Strengthening capacity for monitoring new threats and particularly synthetics through early warning systems and exchange of information. 2) Consolidating balanced approach focusing on humans and strengthening policies for addiction and rehabilitation. 3) Adapting cooperation mechanisms to new reality and use of technology and coordination in the fight´against trafficking and illicit drug flows. Ensuring we can tackle the world drug problem in the spirit of responsibility, solidarity and far from non collaborative approaches that are underscored by ideologies. Stress the importance of the work of the Expert Panel elected by CND. Their recommendations help clarify future discussions leading up to the Ministerial Conference in 2029. We shoulder responsibilities and work with all member states to tackle changing challenges of the world drug problem.
Brunei Darussalam: The global community continues to face challenges across sensitive borders, affecting countries worldwide. Although our national circumstances may vary, we remain vigilant in addressing trafficking methods and emerging trends to support the safety, security, and well-being of our communities. This effort is guided by our national vision for a prosperous, educated, and sustainable nation. Our policies remain responsive to evolving challenges, recognizing that these issues require a coordinated, multi-stakeholder, and inter-institutional response at the highest level. Evidence-based interventions are crucial in this regard. We note recent discussions and proposals to reconsider the classification of cocaine. We reaffirm our position that the coca leaf should remain listed in Schedule I of the Single Convention on Narcotic Drugs of 1961, in accordance with the scientific assessment of its potential for abuse, dependence, and harm to public health. We remain committed to monitoring and combating the abuse and illicit cultivation of narcotic substances.
France: France aligns itself with the statement delivered by the EU on behalf of its MS. Technology is often exploited to increase profits, with traffickers taking advantage of all vulnerabilities, spreading violence, and corrupting institutions. The growing involvement of the most vulnerable minors in trafficking poses a serious threat to their security and future. A new law established a specialized national anti-organized crime department with jurisdiction over interior security forces. High-security units were set up for drug traffickers, and severe sentences are applied to those recruiting minors online. Assets seized from traffickers are reinvested into programs addressing the needs of minors involved in trafficking. Over 30 programs now work in partnership with families, educational systems, social services, internal security forces, and the justice sector to combat trafficking and protect health. Reducing demand is equally important. Our balanced approach focuses on primary prevention, health support, and risk reduction through evidence-based interventions. This includes massive investment in programs proven to reduce psychoactive substance use among young people. These measures are already showing results, with a downward trend in substance use over recent years. Through bilateral relations, we have made drug control a national and international priority. Strengthening cooperation is essential to undermine trafficking, while ensuring that prevention and treatment programs remain aligned with our principles. France opposes the death penalty in all circumstances and emphasizes respect for human rights, calling for strengthened international cooperation. Only by mobilizing states at the highest level, alongside UN agencies, academia, civil society, and the broader society, can we effectively tackle this global phenomenon through a balanced approach.
Lithuania: fully aligns itself with the statements made by the European Union on behalf of the member states. As we meet today, the European context continues to be marked by the consequences of Russia’s war of aggression against Ukraine, military conflicts, and humanitarian crisis hamper the international community’s efforts to be effective. Recent analysis prepared by the European Union Drug Agency shows continuing health and security problems and increasingly, the interplay between them create a challenging policy context for the shaping and implementation of effective response. We should aim to enhance international alliances drug threats and boost preparedness to meet synthetic drugs challenges, we acknowledge the multi disciplinary approach, which emphasizes preparedness, public health, harm reduction and international cooperation, and remains fully committed to collaborating with European Commission member states and all relevant stakeholders to implement the strategy. We understand that drug use continues to pose serious health challenges worldwide, with young people and children affected in the context of addressing risks and harm. Lithuania recognizes the critical importance of harm reduction measures in protecting individuals and communities from the adverse effect of drugs. From January 1st 2027, Lithuania is taking over the Presidency of the Council of the European Union. During presidency, Lithuania will ensure continuity of EU drug policy implementation. We have many reasons to believe in strong international cooperation with different regions of the world to address and counter the world drug problem. We believe that the conventions and UNGASS outcome document enhance the health and wellbeing of humanity. We advocate for pragmatic policies characterized by human centered approaches. Lithuania will continue to uphold nationally and internationally recognized values and rights in the field of drug control policy, remain open to international cooperation and engage in constructive dialogue.
New Zealand: New Zealand takes a health-based, evidence-informed approach to substance use, working closely with the communities most affected. Our health response spans prevention, intensive treatment, and long-term recovery support. Legal and drug-checking services, in partnership with our domestic early warning system, are an important component of this approach. They play a crucial role in intelligence gathering, detecting new substances, and enabling a proactive response to reduce harm in our communities. Over the past two years, we have experienced increased supply and use of methamphetamine, with consumption more than doubling in 2024 alone. We have also seen sustained growth in cocaine use, as well as emerging shifts in our illicit drug landscape, including increased availability of powdered heroin and the detection of automated vaping products. These changes have prompted a rapid, coordinated, cross-government response, focused both on disrupting supply and strengthening our health system’s capacity to reduce demand and address evolving harms. Chair, it is clear that no country can address the challenges of drugs alone. As drug markets expand and associated harms grow, partnership and international cooperation become increasingly important. In this respect, we value the Commission’s leadership and its role as the primary forum. The work of the UN Office on Drugs and Crime and the International Narcotics Control Board not only complements but enhances the success of the Commission. Innovation is another key factor in addressing the drug situation. We must remain open to evidence-based and forward-leaning approaches that advance the core objectives of the international control conventions, safeguarding the health and welfare of humanity. Finally, we are pleased to join today’s discussion on the death penalty. New Zealand considers the death penalty contrary to international law and international consensus.
Isreal: Mr. Chair, I’m honored to represent the experts of the Israel Authority of Community Safety, who are not able to be here due to the ongoing and deliberate Iranian targeting of civilians and civilian infrastructure. These deliberate attacks are committed by Iran and its proxies, aimed at Israel, and indeed, just a few minutes ago, as I saw in reports, targeted Qatar and the UAE. Israel continues to be concerned about the regional trafficking of synthetic drugs, such as Captagon, in the Middle East, and about the use of drug trafficking networks by terrorist organizations, like Iran’s proxies Hezbollah, in order to finance their activities in the region and beyond. If you ask yourself, how does Hezbollah have this money today—$1.2 billion from drugs?—it is instilling not only the freedom of the Lebanese people but also their hard-earned money. The devastating effect of drug abuse is a challenge that spares no nation. Addressing it effectively is not only a public health necessity but also a matter of national security. We’ve adopted a holistic and balanced policy approach that integrates prevention and rehabilitation and enforcement. Our policy is rooted in the understanding that substance use is a widespread social and public health issue requiring coordinated community-wide action. We recognize the essential role of local and municipal authorities as key partners, and equip them with evidence-based knowledge, tools, and resources to ensure a continuation of care—from early identification to rehabilitation and reintegration—tailored to the specific needs of each community. Recent global experiences have shown that periods of distress, instability, and crisis—such as Israel and Israelis are going through as we speak, with targeted missile attacks on civilian areas—significantly affect patterns of substance use and access to care. Concerning trends in Israel indicate the need to protect vulnerable populations during times of crisis. In this context, I would like to invite everyone to our side event on trauma, psychoactive substance use and integrated care, the case of NOVA survivors hosted by Israel with support from Germany tomorrow on March 11 1pm to 2pm at Room M3. During the event, we will share Israel’s drawing on the case of the survivors of the Palestinian Hamas terrorist organization massacre at the NOVA Festival. Israel’s drug policy is grounded in a comprehensive people centered approach that places health and well-being at its core, adapting programs to gender, age and culture sensitivities and ensuring high risk groups, including young detainees, receive appropriate support. We are currently implementing a structural reform to strengthen the addiction treatment system by transferring responsibility for these services to health maintenance organizations. We aim to reduce stigma, improve accessibility and ensure person centered care for all our individuals in need. The global challenge of drug abuse requires a global commitment and shared responsibilities to exchange information, share best practices, and strengthen cooperation in order to build a resilient, inclusive and effective response to this complex issue.
Afghanistan: Since the Taliban takeover in August 2021, the drug situation in Afghanistan has deteriorated. While the Taliban claimed to have abandoned poppy cultivation, available evidence indicates that enforcement has been selective and inconsistent. Rather than dismantling the economy, these measures enabled the consolidation control over stockpiles, influence supply chains, and drive financial and political leverage.According to recent UNODC assessment, we remain a critical concern in the global drug landscape and indicate a shift from traditional narcotics to synthetic drugs particularly methamphetamine. The problem is easy to conceal, profitable and poses serious risk to public health, regional stability and international security. The drug problem cannot be separated from the broader crisis of governance, accountability and human rights. Systematic restrictions such as exclusion of women and girls from education, employment, and public life undermine social resilience, and weaken the foundation necessary for sustainable counternarcotic force. Female drug addiction in Afghanistan is a serious but often underreported problem. Research and reports estimate that Afghanistan has about 2 to 3.6 million drug users with around 850.000 to 1 million women and children affected. In addition to illicit drugs, the people of Afghanistan are also suffering from large scale, illegal, and systematically organized extraction of natural resources, particularly in Northern and North Eastern Afghanistan, conducted outside any legal framework, these activities constitute environmental crimes linked to organized criminal networks. The resulting land degradation, water contamination, and ecological destruction exacerbate suffering and undermine long term stability. In this context, we urge the international community to refrain from legitimizing measures by the Taliban to continuously support international accountability mechanisms and to ensure that humanitarian and development assistance reaches the people of Afghanistan. A sustainable and effective response to the drug program requires long term commitment, regional cooperation, and conditions that support inclusive government, the rule of law, and respect for fundamental rights.
Chair: I would like to thank interpreters for agreeing to continue our services until 13.10, this is very helpful. With this, I have the pleasure to give the floor to Nigeria
Nigeria: Over 292 million people worldwide used drugs past year, representing a continued upward trend. The report highlights a rapid expansion of synthetic drug markets, particularly synthetic opioids and a growing adaptability of organized criminal networks and record levels of cocaine production, and an increasing complex trafficking networks spanning multiple jurisdictions. Nigeria remains resolute in addressing this challenge under the concluding phase of the National Drug Control Master Plan. We have sustained a balanced strategy combining supply reduction, demand reduction, and harm reduction measures. These achievements reflect intensified interdiction operation intelligence and strengthened interagency cooperation. As we approach the end of the current master plan cycle, Nigeria has commenced to work on a new draft 2026-2030. The forthcoming framework will consolidate license land, integrate global trends from 2025 world drug report, and place greater emphasis on synthetic drugs control disruption of drug economy, digital trafficking channels, and sustainable community resilience. Nigeria is committed to evidence based intervention, addressing the health and social consequences of drugs. The war against drug abuse remains central to our whole of society approach, by mobilizing youth, traditional rulers, religious leaders, and women’s groups and civil society actors nationwide. This structure extends from the national, Interministerial Drug Control Committee to sub national state level to local governments and community drug control committees. In the area of alternative development, the agency has expanded livelihood support programs to encourage leadership and economic resilience. It also addresses the microeconomic roots that sustain illicit cultivation. Introduces preventive human strategy. Community based agricultural and vocational initiatives have been implemented. We met progress in discouraging cannabis cultivation and promoting lawful income generating activities. Medicine cannabis remains widely used and the 2025 world drug report confirms its global prevalence and rising potencies. Synthetic opioids, particularly tramadol, still poses serious challenges in Nigeria. Why not schedule it internationally? Its non medical use and cross border trafficking require international cooperation and improved precursor monitoring. We remain committed to international drug control conventions and to collaborative, balanced and humane responses to the evolving world drug problem.
Tanzania: We align with the African Group and G77 and China. We stand at a pivot conjecture confronted by opportunities and responsibilities. Our location poses us as a support hub and we are integral to global response to illicit drugs. As many other nations we have an evolving and complex drug phenomenon including traditional drug markets, increased domestic consumption, synthetic substances and misuse of prescription medication and highly organized trafficking networks with advanced technology. We underscore the need to reduce supply, implement measures to curb demand and enhance harm reduction. We commit to protect public health, uphold human rights and foster sustainable development. We learned some lessons that we will share and seek support from the international community. We have a policy framework that ensures coherence across ministries of health, justice, security, social welfare, development. Our national drug control strategy is balanced and includes law enforcement, evidence-based treatment and harm reduction services, prevention, education, community resilience and social integration. Our drug control enforcement authority was improved as a coordinating body to enhance interagency cooperation and international partnerships. We have supply reduction and law enforcement measures to dismantle criminal networks, not only couriers but also the masterminds and the supply of chemical precursors. Our measures include maritime control, border control, customs profiling, and improved intelligence shared with international partners. Our laboratory capacities and forensic capacity expanded to support investigation and enable us to identify emerging substances. We seized 107472 tons of various drugs. We firmly believe that demand reduction, treatment and harm reduction are fundamental to effective public health responses. We expanded access to evidence-based prevention, community outreach, treatment services and psychosocial support. Drug dependence treatment services have been created in all mental health and substance use units with 2900 individuals in treatment, 17 medication assisted sites who serve 18048 patients and 77 recovery homes supporting 4396 individuals and 4700 people who inject drugs in needle and syringe programmes . Our initiatives include pragmatic measures to reduce mortality and disease transmission while linking people to treatment and social services. We expanded gender responsive treatment so that intervention does not further marginalized vulnerable populations. We recognize the importance of prevention and youth engagement and community resilience. In 2025 we reached our 3million primary school children with evidence-based prevention education. Drug trafficking and organized crime are transnational issues that necessitate coordinated responses through regional international collaboration. Tanzania actively participates in regional mechanisms, collaborates with neighboring states, and engages multilaterally with the UNODC and other relevant national partners.Our cooperation encompasses operational coordination, training exchanges, joint operations and legal assistance. We highly value the technical assistance we receive from the United Nations and bilateral partners which have been instrumental in accelerating our progress amid evolving threats. However, despite these great positive progress registered, we continue to face significant challenges including inadequate technology for intelligence led policy policing, forensic analysis, supply chain monitoring. The rise of online trafficking and abuse of digital platforms alongside synthetic drugs and new psychoactive substances post serious concerns. Resources constraints and the ongoing need for specialized straining and laboratory capacity building remain barriers we are committed to address. We must reaffirm our commitment to our balanced evidence based and humane response to the drug problem. We call for 4 issues 1) sustainable and predictable international support for capacity building and forensics science, early warning systems treatment expansion and community programs, 2) strengthened international cooperation on precursor financial investigation measures to disrupt digital platforms, facilitate and trafficking, 3)exchange of best practices into operational lessons 4) collaborating research to understand and respond to synthetic drugs, scale up effective harm reduction where appropriate, and evaluate. There is no single solution to the complex evolving drug problem, only a multisectoral and balanced approach combining effective law enforcement, public health, protection of human rights, sustainable development to ensure safety, health and opportunities to our citizens. I look forward to constructive dialogue and cooperation in our collective efforts to address the drug problem. I invite you all to our side event on countering the outcoming threats, realities of synthetic drugs and precursor trafficking in east africa.
Chair: That brings us to the end of this meeting. We continue with general debate at 3pm with Malaysia and Greece. If time permits, at the end of the day we resume agenda item 5.